

Comparison of trends in tuberculosis incidence among adults living with HIV and adults without HIV--Kenya, 1998-2012
- PMID: 24937804
- PMCID: PMC4061026
- DOI: 10.1371/journal.pone.0099880
Comparison of trends in tuberculosis incidence among adults living with HIV and adults without HIV--Kenya, 1998-2012
Abstract
Background: In Kenya, the comparative incidences of tuberculosis among persons with and without HIV have not been described, and the differential impact of public health interventions on tuberculosis incidence in the two groups is unknown.
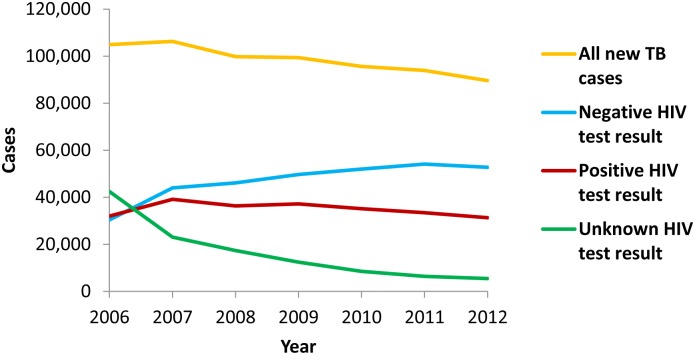
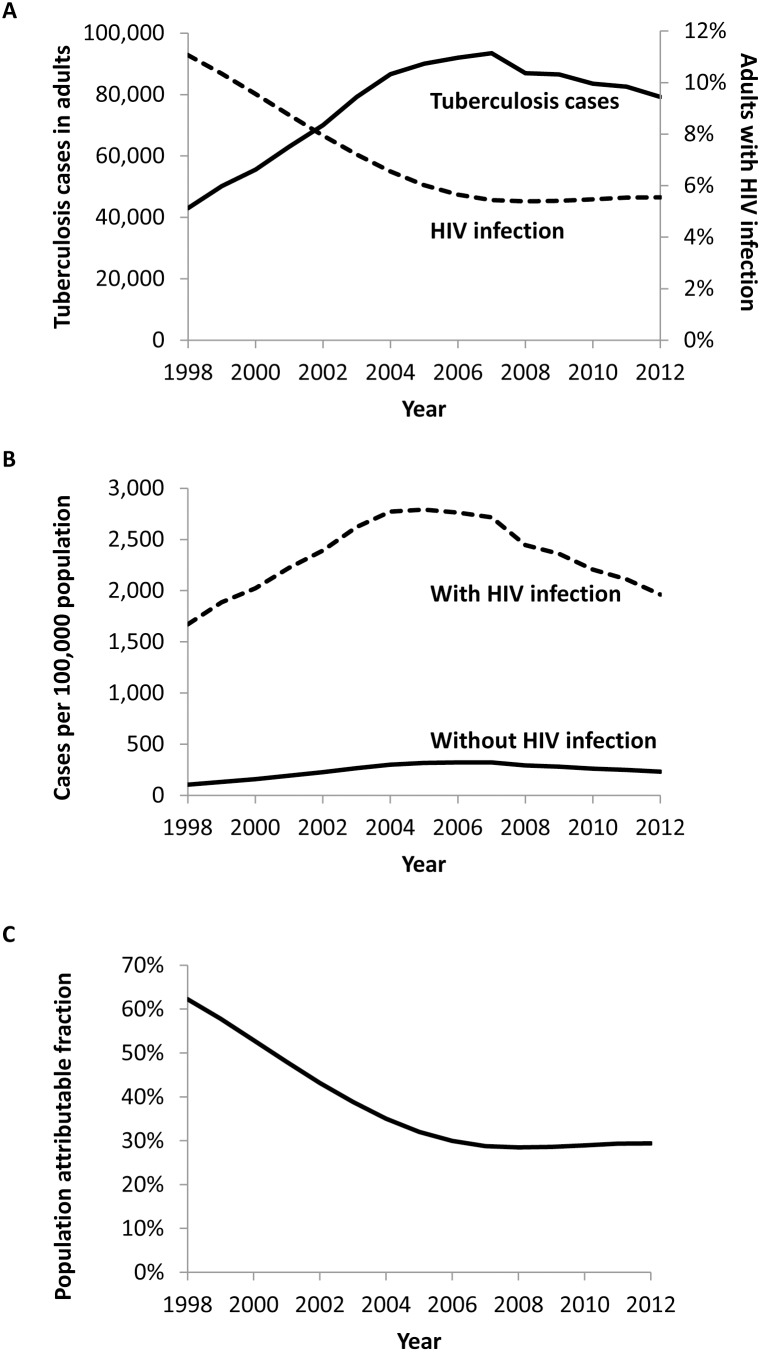
Methods: We estimated annual tuberculosis incidence stratified by HIV status during 2006-2012 based on the numbers of reported tuberculosis patients with and without HIV infection, the prevalence of HIV infection in the general population, and the total population. We also made crude estimates of annual tuberculosis incidence stratified by HIV status during 1998-2012 by assuming a constant ratio of HIV prevalence among tuberculosis patients compared to the general population.
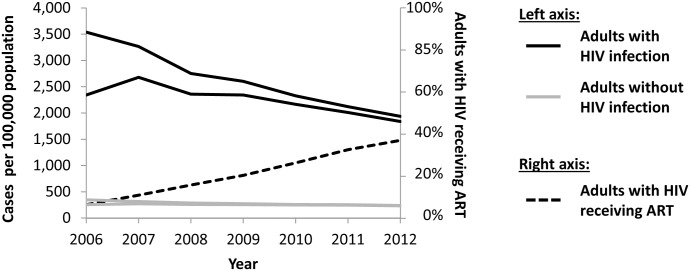
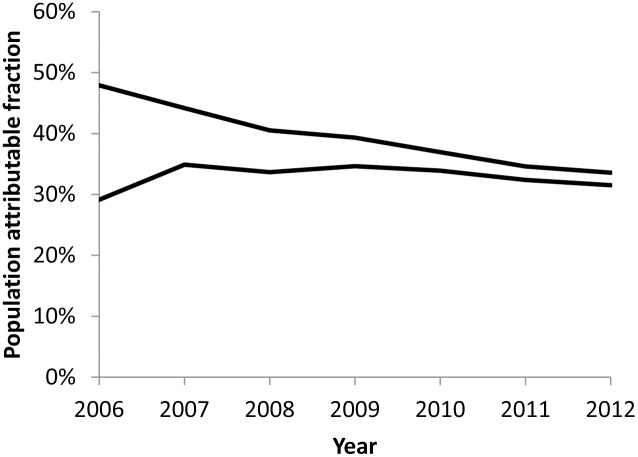
Results: Tuberculosis incidence among both adults with HIV and adults without HIV increased during 1998-2004 then remained relatively stable until 2007. During 2007-2012, tuberculosis incidence declined by 28-44% among adults with HIV and by 11-26% among adults without HIV, concurrent with an increase in antiretroviral therapy uptake. In 2012, tuberculosis incidence among adults with HIV (1,839-1,936 cases/100,000 population) was still eight times as high as among adults without HIV (231-238 cases/100,000 population), and approximately one third of tuberculosis cases were attributable to HIV.
Conclusions: Although tuberculosis incidence has declined among adults with and without HIV, the persistent high incidence of tuberculosis among those with HIV and the disparity between the two groups are concerning. Early diagnosis of HIV, early initiation of antiretroviral therapy, regular screening for tuberculosis, and isoniazid preventive therapy among persons with HIV, as well as tuberculosis control in the general population, are required to address these issues.
Conflict of interest statement
Figures
References
-
- World Health Organization (2013) Global tuberculosis report 2013. Geneva: World Health Organization.
-
- van’t Hoog AH, Williamson J, Sewe M, Mboya P, Odeny LO, et al. (2012) Risk factors for excess mortality and death in adults with tuberculosis in Western Kenya. Int J Tuberc Lung Dis 16: 1649–1656. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
