

Vitamin D and mortality: meta-analysis of individual participant data from a large consortium of cohort studies from Europe and the United States
- PMID: 24938302
- PMCID: PMC4061380
- DOI: 10.1136/bmj.g3656
Vitamin D and mortality: meta-analysis of individual participant data from a large consortium of cohort studies from Europe and the United States
Abstract
Objective: To investigate the association between serum 25-hydroxyvitamin D concentrations (25(OH)D) and mortality in a large consortium of cohort studies paying particular attention to potential age, sex, season, and country differences.
Design: Meta-analysis of individual participant data of eight prospective cohort studies from Europe and the US.
Setting: General population.
Participants: 26,018 men and women aged 50-79 years.
Main outcome measures: All-cause, cardiovascular, and cancer mortality.
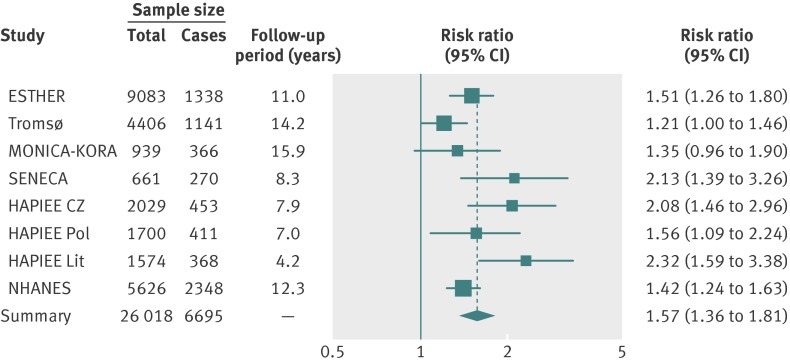
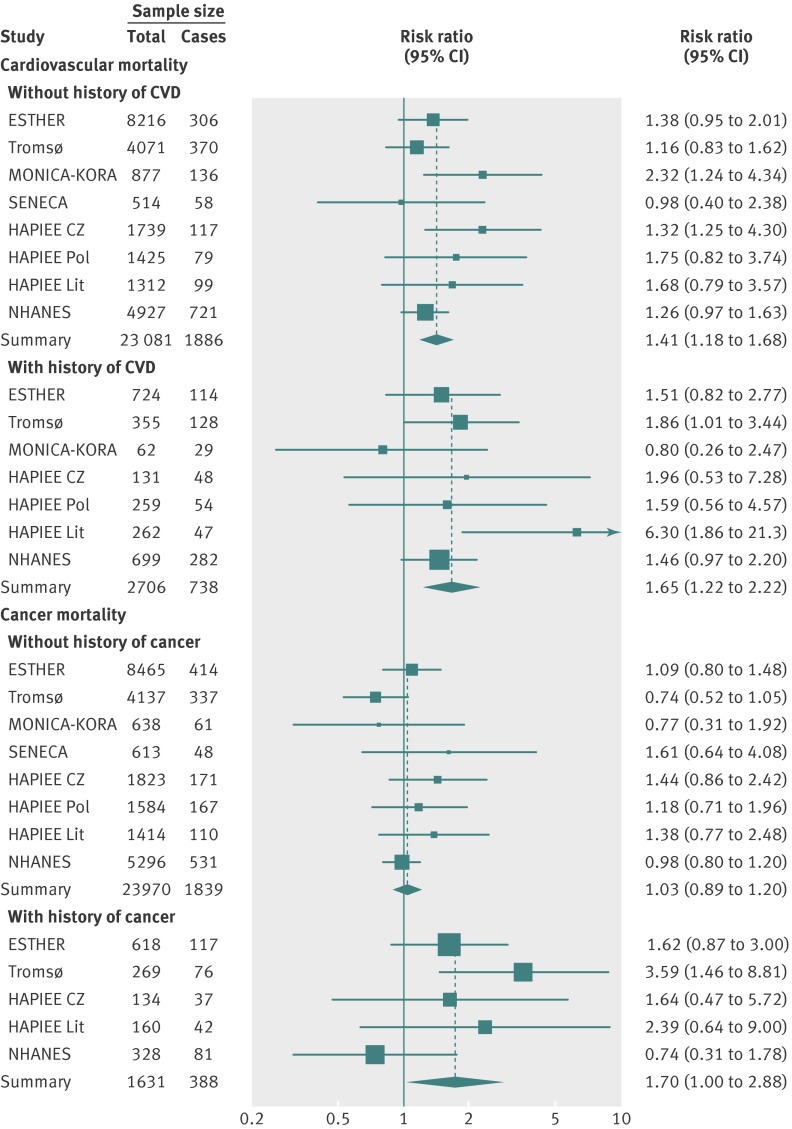
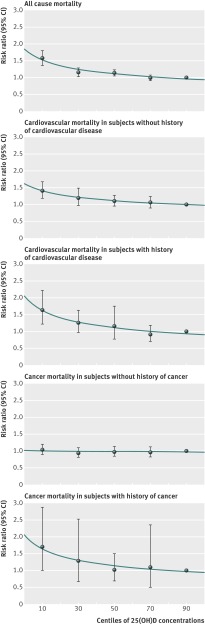
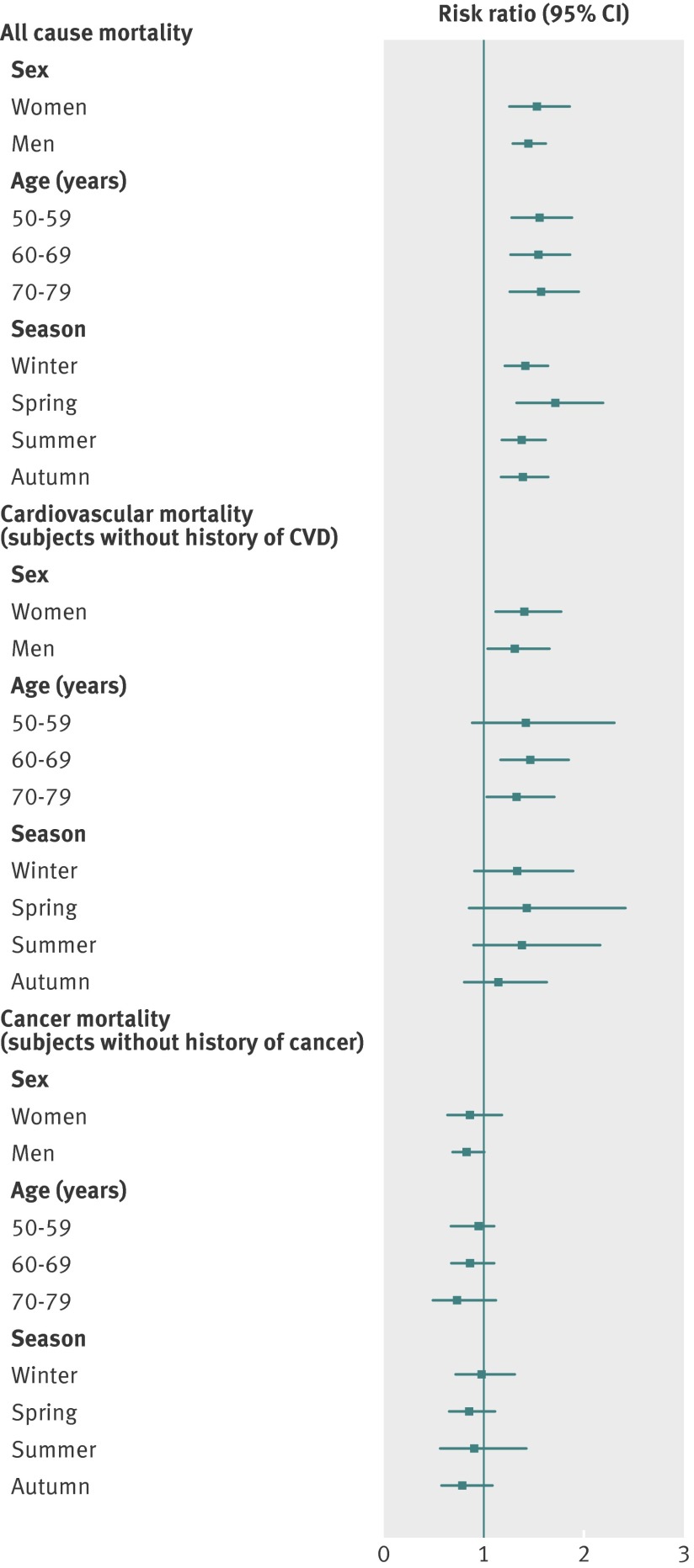
Results: 25(OH)D concentrations varied strongly by season (higher in summer), country (higher in US and northern Europe) and sex (higher in men), but no consistent trend with age was observed. During follow-up, 6695 study participants died, among whom 2624 died of cardiovascular diseases and 2227 died of cancer. For each cohort and analysis, 25(OH)D quintiles were defined with cohort and subgroup specific cut-off values. Comparing bottom versus top quintiles resulted in a pooled risk ratio of 1.57 (95% CI 1.36 to 1.81) for all-cause mortality. Risk ratios for cardiovascular mortality were similar in magnitude to that for all-cause mortality in subjects both with and without a history of cardiovascular disease at baseline. With respect to cancer mortality, an association was only observed among subjects with a history of cancer (risk ratio, 1.70 (1.00 to 2.88)). Analyses using all quintiles suggest curvilinear, inverse, dose-response curves for the aforementioned relationships. No strong age, sex, season, or country specific differences were detected. Heterogeneity was low in most meta-analyses.
Conclusions: Despite levels of 25(OH)D strongly varying with country, sex, and season, the association between 25(OH)D level and all-cause and cause-specific mortality was remarkably consistent. Results from a long term randomised controlled trial addressing longevity are being awaited before vitamin D supplementation can be recommended in most individuals with low 25(OH)D levels.
© Schöttker et al 2014.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Are trials of vitamin D with mortality as an endpoint really needed?BMJ. 2014 Jul 9;349:g4452. doi: 10.1136/bmj.g4452. BMJ. 2014. PMID: 25008347 No abstract available.
References
-
- Zerwekh JE. Blood biomarkers of vitamin D status. Am J Clin Nutr 2008;87:1087S-91S. - PubMed
-
- van der Wielen RP, Löwik MR, van den Berg H, de Groot LC, Haller J, Moreiras O, et al. Serum vitamin D concentrations among elderly people in Europe. Lancet 1995;346:207-10. - PubMed
-
- Chang EM, Kim YS, Won HJ, Yoon TK, Lee WS. Association between sex steroids, ovarian reserve, and vitamin D levels in healthy non-obese women. J Clin Endocrinol Metab 2014:jc20133873. - PubMed
-
- Mosekilde L. Vitamin D and the elderly. Clin Endocrinol (Oxf) 2005;62:265-81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical