

Impact of patient navigation on timely cancer care: the Patient Navigation Research Program
- PMID: 24938303
- PMCID: PMC4072900
- DOI: 10.1093/jnci/dju115
Impact of patient navigation on timely cancer care: the Patient Navigation Research Program
Abstract
Background: Patient navigation is a promising intervention to address cancer disparities but requires a multisite controlled trial to assess its effectiveness.
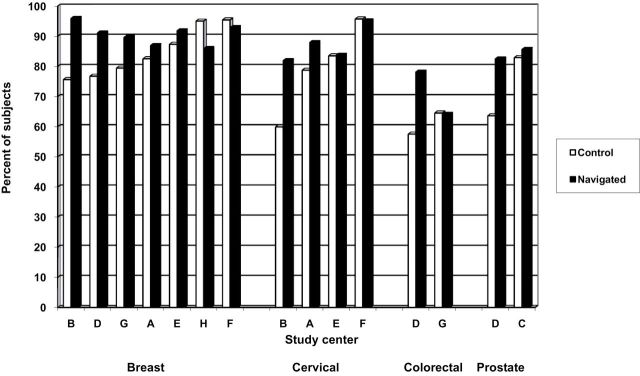
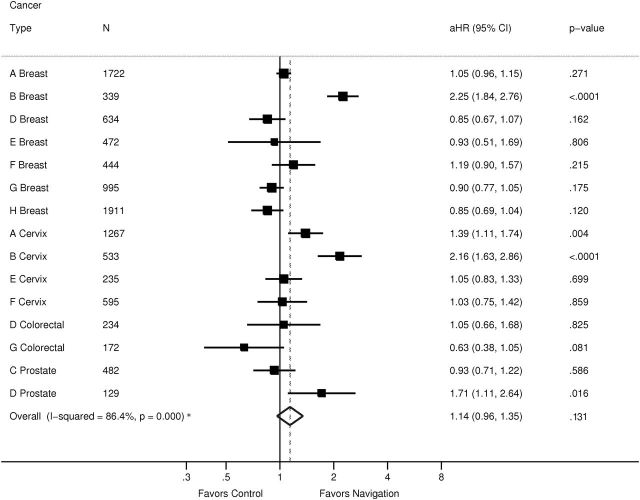
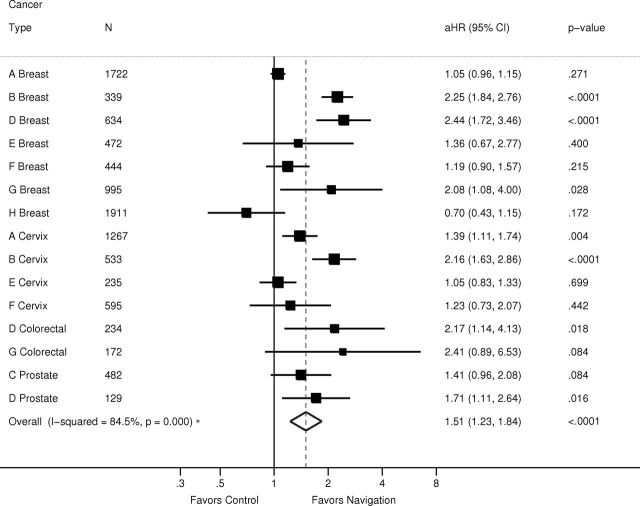
Methods: The Patient Navigation Research Program compared patient navigation with usual care on time to diagnosis or treatment for participants with breast, cervical, colorectal, or prostate screening abnormalities and/or cancers between 2007 and 2010. Patient navigators developed individualized strategies to address barriers to care, with the focus on preventing delays in care. To assess timeliness of diagnostic resolution, we conducted a meta-analysis of center- and cancer-specific adjusted hazard ratios (aHRs) comparing patient navigation vs usual care. To assess initiation of cancer therapy, we calculated a single aHR, pooling data across all centers and cancer types. We conducted a metaregression to evaluate variability across centers. All statistical tests were two-sided.
Results: The 10521 participants with abnormal screening tests and 2105 with a cancer or precancer diagnosis were predominantly from racial/ethnic minority groups (73%) and publically insured (40%) or uninsured (31%). There was no benefit during the first 90 days of care, but a benefit of navigation was seen from 91 to 365 days for both diagnostic resolution (aHR = 1.51; 95% confidence interval [CI] = 1.23 to 1.84; P < .001)) and treatment initiation (aHR = 1.43; 95% CI = 1.10 to 1.86; P < .007). Metaregression revealed that navigation had its greatest benefits within centers with the greatest delays in follow-up under usual care.
Conclusions: Patient navigation demonstrated a moderate benefit in improving timely cancer care. These results support adoption of patient navigation in settings that serve populations at risk of being lost to follow-up.
© The Author 2014. Published by Oxford University Press. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- American College of Surgeons. National Accrediation Program for Breast Centers Breast Center Components Chicago: American College of Surgeons; 2010. http://accreditedbreastcenters.org/standards/standards.html Accessed November 21, 2010
-
- National Comprehensive Cancer Network. The case manager or patient navigator: providing support for cancer patients during treatment and beyond National Comprehensive Cancer Network. http://www.nccn.com/living-with-cancer/understanding-treatment/152-case-... Accessed April 16, 2014
-
- Robinson-White S, Conroy B, Slavish KH, Rosenzweig M. Patient navigation in breast cancer: a systematic review. Cancer Nurs. 2010;33(2):127–140 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
