

Effect of selumetinib vs chemotherapy on progression-free survival in uveal melanoma: a randomized clinical trial
- PMID: 24938562
- PMCID: PMC4249701
- DOI: 10.1001/jama.2014.6096
Effect of selumetinib vs chemotherapy on progression-free survival in uveal melanoma: a randomized clinical trial
Abstract
Importance: Uveal melanoma is characterized by mutations in GNAQ and GNA11, resulting in mitogen-activated protein kinase pathway activation.
Objective: To assess the efficacy of selumetinib, a selective, non-adenosine triphosphate competitive inhibitor of MEK1 and MEK2, in uveal melanoma.
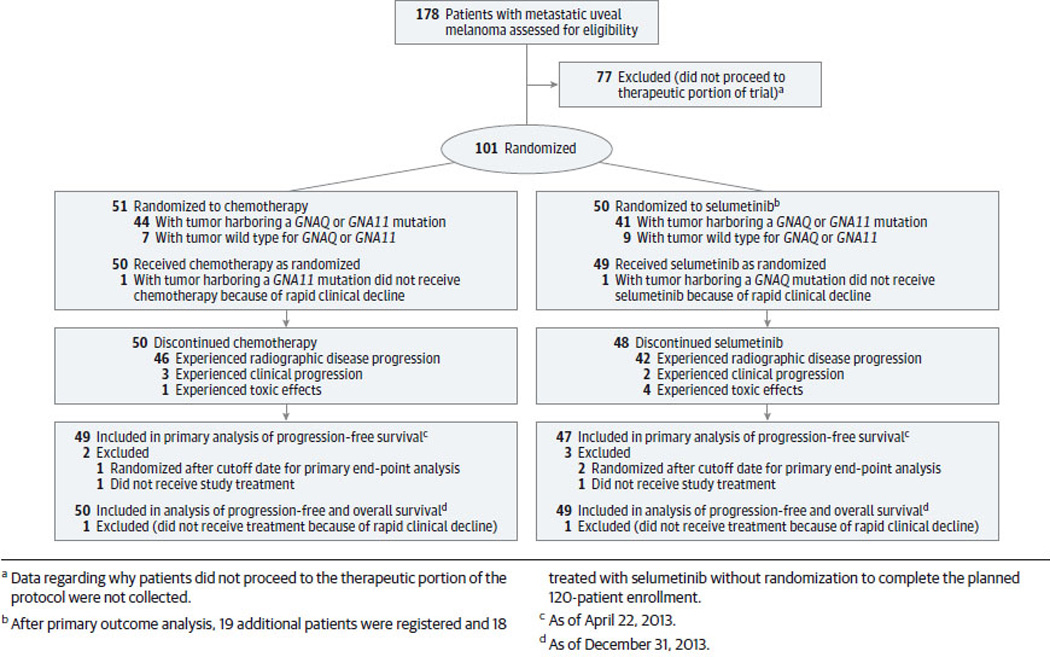
Design, setting, and participants: Randomized, open-label, phase 2 clinical trial comparing selumetinib vs chemotherapy conducted from August 2010 through December 2013 among 120 patients with metastatic uveal melanoma at 15 academic oncology centers in the United States and Canada.
Interventions: One hundred one patients were randomized in a 1:1 ratio to receive selumetinib, 75 mg orally twice daily on a continual basis (n = 50), or chemotherapy (temozolomide, 150 mg/m2 orally daily for 5 of every 28 days, or dacarbazine, 1000 mg/m2 intravenously every 21 days [investigator choice]; n = 51) until disease progression, death, intolerable adverse effects, or withdrawal of consent. After primary outcome analysis, 19 patients were registered and 18 treated with selumetinib without randomization to complete the planned 120-patient enrollment. Patients in the chemotherapy group could receive selumetinib at the time of radiographic progression.
Main outcomes and measures: Progression-free survival, the primary end point, was assessed as of April 22, 2013. Additional end points, including overall survival, response rate, and safety/toxicity, were assessed as of December 31, 2013.
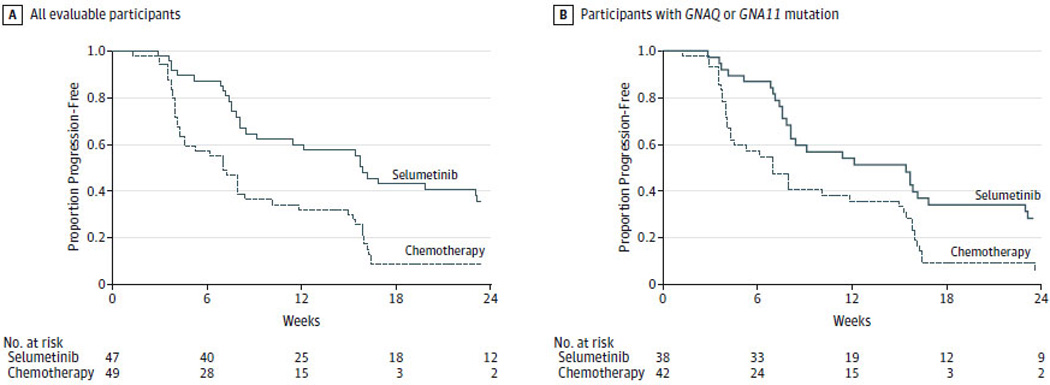
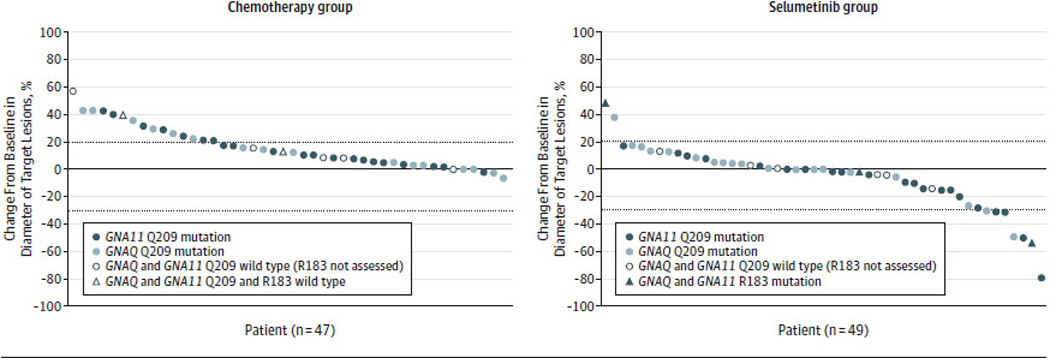
Results: Median progression-free survival among patients randomized to chemotherapy was 7 weeks (95% CI, 4.3-8.4 weeks; median treatment duration, 8 weeks; interquartile range [IQR], 4.3-16 weeks) and among those randomized to selumetinib was 15.9 weeks (95% CI, 8.4-21.1 weeks; median treatment duration, 16.1 weeks; IQR, 8.1-25.3 weeks) (hazard ratio, 0.46; 95% CI, 0.30-0.71; P < .001). Median overall survival time was 9.1 months (95% CI, 6.1-11.1 months) with chemotherapy and 11.8 months (95% CI, 9.8-15.7 months) with selumetinib (hazard ratio, 0.66; 95% CI, 0.41-1.06; P = .09). No objective responses were observed with chemotherapy. Forty-nine percent of patients treated with selumetinib achieved tumor regression, with 14% achieving an objective radiographic response to therapy. Treatment-related adverse events were observed in 97% of patients treated with selumetinib, with 37% requiring at least 1 dose reduction.
Conclusions and relevance: In this hypothesis-generating study of patients with advanced uveal melanoma, selumetinib compared with chemotherapy resulted in a modestly improved progression-free survival and response rate; however, no improvement in overall survival was observed. Improvement in clinical outcomes was accompanied by a high rate of adverse events.
Trial registration: clinicaltrials.gov Identifier: NCT01143402.
Figures
Comment in
-
Uveal melanoma therapy on the horizon?Cancer Discov. 2014 Sep;4(9):OF6. doi: 10.1158/2159-8290.CD-NB2014-103. Epub 2014 Jul 9. Cancer Discov. 2014. PMID: 25185205
References
-
- Chang AE, Karnell LH, Menck HR. The National Cancer Data Base report on cutaneous and noncutaneous melanoma: a summary of 84,836 cases from the past decade. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer. 1998 Oct 15;83(8):1664–1678. - PubMed
-
- Singh AD, Topham A. Incidence of uveal melanoma in the United States: 1973–1997. Ophthalmology. 2003 May;110(5):956–961. - PubMed
-
- Assessment of metastatic disease status at death in 435 patients with large choroidal melanoma in the Collaborative Ocular Melanoma Study (COMS): COMS report no. 15. Arch Ophthalmol. 2001 May;119(5):670–676. - PubMed
-
- Rietschel P, Panageas KS, Hanlon C, Patel A, Abramson DH, Chapman PB. Variates of survival in metastatic uveal melanoma. J Clin Oncol. 2005 Nov 1;23(31):8076–8080. - PubMed
-
- Diener-West M, Reynolds SM, Agugliaro DJ, et al. Development of metastatic disease after enrollment in the COMS trials for treatment of choroidal melanoma: Collaborative Ocular Melanoma Study Group Report No. 26. Arch Ophthalmol. 2005 Dec;123(12):1639–1643. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
