

Neurological adverse events in patients receiving anti-TNF therapy: a prospective imaging and electrophysiological study
- PMID: 24938855
- PMCID: PMC4229940
- DOI: 10.1186/ar4582
Neurological adverse events in patients receiving anti-TNF therapy: a prospective imaging and electrophysiological study
Abstract
Introduction: The aim was to investigate the frequency of neurological adverse events in patients with rheumatoid arthritis (RA) and spondylarthropathies (SpA) treated with tumor necrosis factor (TNF) α antagonists.
Methods: Seventy-seven patients eligible for anti-TNFα therapy were evaluated. There were 36 patients with RA, 41 with SpA [24 psoriatic arthritis (PsA) and 17 with ankylosing spondylitis (AS)]. All patients had a complete physical and neurological examination. Brain and cervical spine magnetic resonance imaging (MRI) and neurophysiological tests were performed in all patients before the initiation of anti-TNFα therapy and after a mean of 18 months or when clinical symptoms and signs indicated a neurological disease. Exclusion criteria included hypertension, diabetes mellitus, dyslipidemia, heart arrhythmias, atherothrombotic events, vitamin B12 and iron deficiency, head and neck trauma and neurological surgeries.
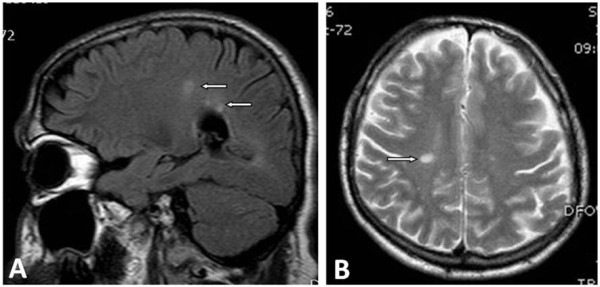
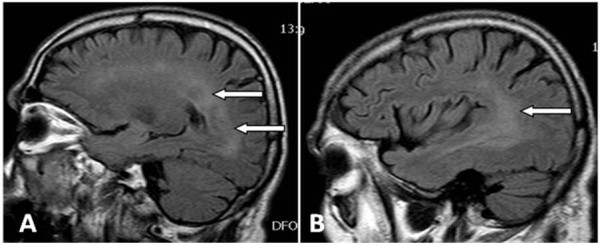
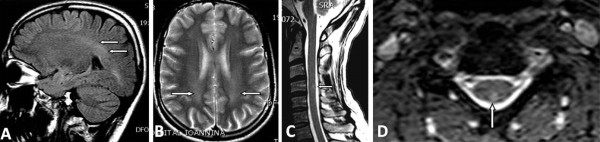
Results: Two patients did not receive anti-TNFα therapy because brain MRIs at baseline revealed lesions compatible with demyelinating diseases. Thus, 75 patients received anti-TNFα (38 infliximab, 19 adalimumab and 18 etanercept). Three patients developed neurological adverse events. A 35-year-old man with PsA after 8 months of infliximab therapy presented with paresis of the left facial nerve and brain MRI showed demyelinating lesions. Infliximab was discontinued and he was treated with pulses of corticosteroids recovering completely after two months. The second patient was a 45-year-old woman with RA who after 6 months of adalimumab therapy presented with optic neuritis. The third patient was a 50-year-old woman with AS, whom after 25 months of infliximab therapy, presented with tingling and numbness of the lower extremities and neurophysiological tests revealed peripheral neuropathy. In both patients anti-TNF were discontinued and they improved without treatment after 2 months. The rest of our patients showed no symptoms and MRIs showed no abnormalities. The estimated rate of neurological adverse events in patients treated with anti-TNF therapy is 4% (3/75).
Conclusions: Neurological adverse events after anti-TNFα therapy were observed in our patient. Brain MRI and neurophysiological tests are essential tools to discriminate neurological diseases.
Figures
References
-
- Voulgari PV, Alamanos Y, Nikas SN, Bougias DV, Temekonidis TI, Drosos AA. Infliximab therapy in established rheumatoid arthritis: an observational study. Am J Med. 2005;118:515–520. - PubMed
-
- Voulgari PV, Venetsanopoulou AI, Exarchou SA, Alamanos Y, Tsifetaki N, Drosos AA. Sustained clinical response and high infliximab survival in psoriatic arthritis patients: a 3-year long-term study. Semin Arthritis Rheum. 2008;37:293–298. - PubMed
-
- Saougou I, Markatseli TE, Voulgari PV, Drosos AA. Maintained clinical response of infliximab treatment in ankylosing spondylitis: a 6-year long-term study. Joint Bone Spine. 2010;77:325–329. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
