

Triggers and treatment of anaphylaxis: an analysis of 4,000 cases from Germany, Austria and Switzerland
- PMID: 24939374
- PMCID: PMC4075276
- DOI: 10.3238/arztebl.2014.0367
Triggers and treatment of anaphylaxis: an analysis of 4,000 cases from Germany, Austria and Switzerland
Abstract
Background: Anaphylaxis is the most severe manifestation of a mast cell-dependent immediate reaction and may be fatal. According to data from the Berlin region, its incidence is 2-3 cases per 100 000 persons per year.
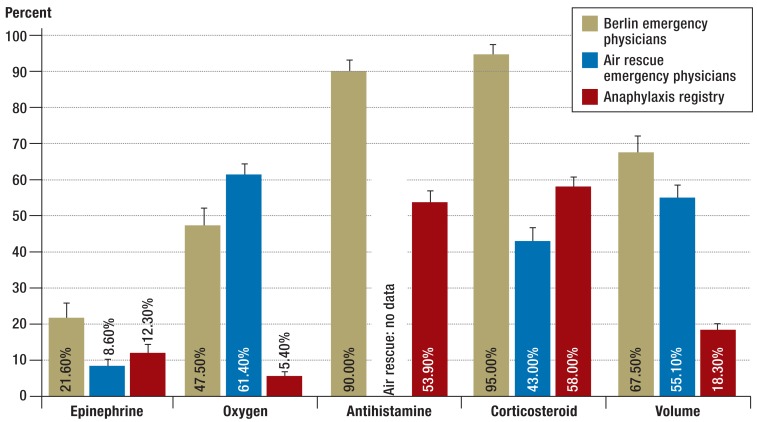
Method: We evaluated data from the anaphylaxis registry of the German-speaking countries for 2006-2013 and data from the protocols of the ADAC air rescue service for 2010-2011 to study the triggers, clinical manifestations, and treatment of anaphylaxis.
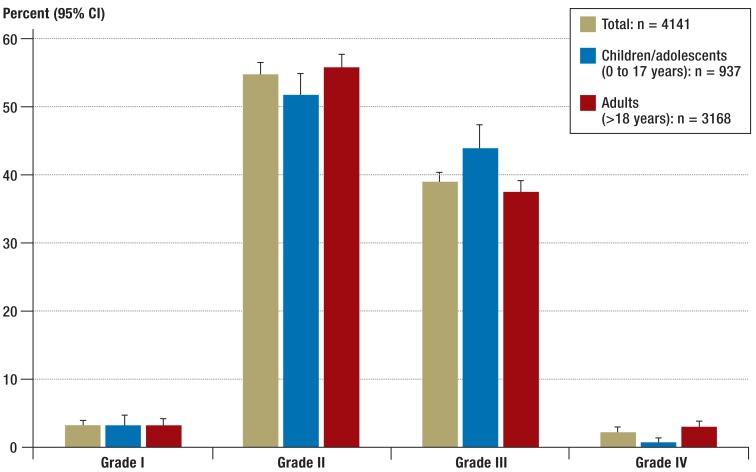
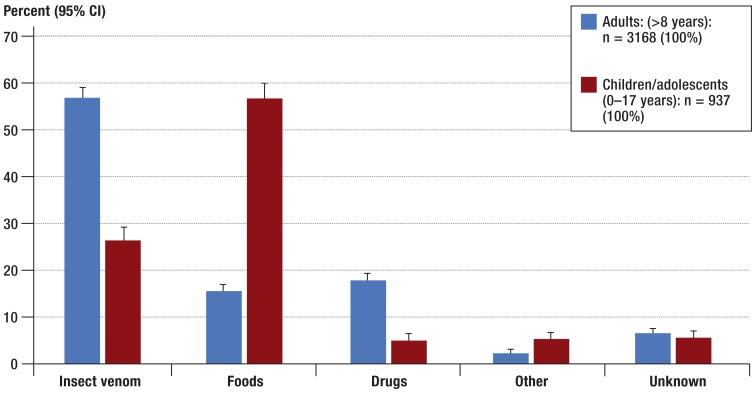
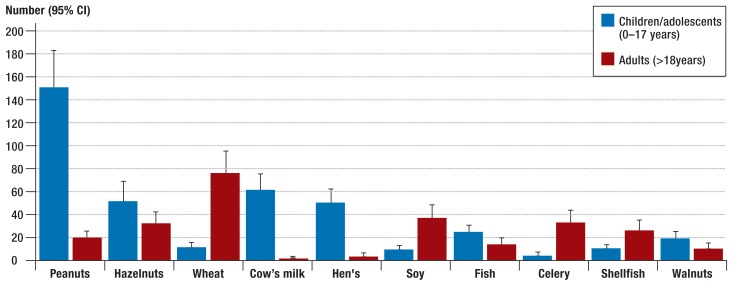
Results: The registry contained data on 4141 patients, and the ADAC air rescue protocols concerned 1123 patients. In the registry, the most common triggers for anaphylaxis were insect venom (n = 2074; 50.1%), foods (n = 1039; 25.1%), and drugs (n = 627; 15.1%). Within these groups, the most common triggers were wasp (n = 1460) and bee stings (n = 412), legumes (n = 241), animal proteins (n = 225), and analgesic drugs (n = 277). Food anaphylaxis was most frequently induced by peanuts, cow milk, and hen's egg in children and by wheat and shellfish in adults. An analysis of the medical emergency cases revealed that epinephrine was given for grade 3 or 4 anaphylaxis to 14.5% and 43.9% (respectively) of the patients in the anaphylaxis registry and to 19% and 78% of the patients in the air rescue protocols.
Conclusion: Wasp and bee venom, legumes, animal proteins, and analgesic drugs were the commonest triggers of anaphylaxis. Their relative frequency was age-dependent. Epinephrine was given too rarely, as it is recommended in the guidelines for all cases of grade 2 and above.
Figures
Comment in
-
Adrenaline as the medication of choice.Dtsch Arztebl Int. 2015 Jan 23;112(4):59. doi: 10.3238/arztebl.2015.0059a. Dtsch Arztebl Int. 2015. PMID: 25797424 Free PMC article. No abstract available.
-
Not all legumes are triggers.Dtsch Arztebl Int. 2015 Jan 23;112(4):59. doi: 10.3238/arztebl.2015.0059b. Dtsch Arztebl Int. 2015. PMID: 25797425 Free PMC article. No abstract available.
-
In reply.Dtsch Arztebl Int. 2015 Jan 23;112(4):59. doi: 10.3238/arztebl.2015.0059c. Dtsch Arztebl Int. 2015. PMID: 25797426 Free PMC article. No abstract available.
References
-
- Johansson SG, Bieber T, Dahl R, et al. Revised nomenclature for allergy for global use: Report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. J Allergy Clin Immunol. 2004;113:832–836. - PubMed
-
- Ring J, Grosber M, Mohrenschlager M, Brockow K. Anaphylaxis: acute treatment and management. Chem Immunol Allergy. 2010;95:201–210. - PubMed
-
- Simons FE, Ardusso LR, Bilo MB, et al. World Allergy Organization anaphylaxis guidelines: summary. J Allergy Clin Immunol. 2011;127:587–593. e1-22. - PubMed
-
- Ring J, Messmer K. Incidence and severity of anaphylactoid reactions to colloid volume substitutes. Lancet. 1977;1:466–469. - PubMed
-
- Sampson HA, Munoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: summary report-Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol. 2006;117:391–397. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical