

The impact and cost of scaling up midwifery and obstetrics in 58 low- and middle-income countries
- PMID: 24941336
- PMCID: PMC4062394
- DOI: 10.1371/journal.pone.0098550
The impact and cost of scaling up midwifery and obstetrics in 58 low- and middle-income countries
Abstract
Background and methods: To guide achievement of the Millennium Development Goals, we used the Lives Saved Tool to provide a novel simulation of potential maternal, fetal, and newborn lives and costs saved by scaling up midwifery and obstetrics services, including family planning, in 58 low- and middle-income countries. Typical midwifery and obstetrics interventions were scaled to either 60% of the national population (modest coverage) or 99% (universal coverage).
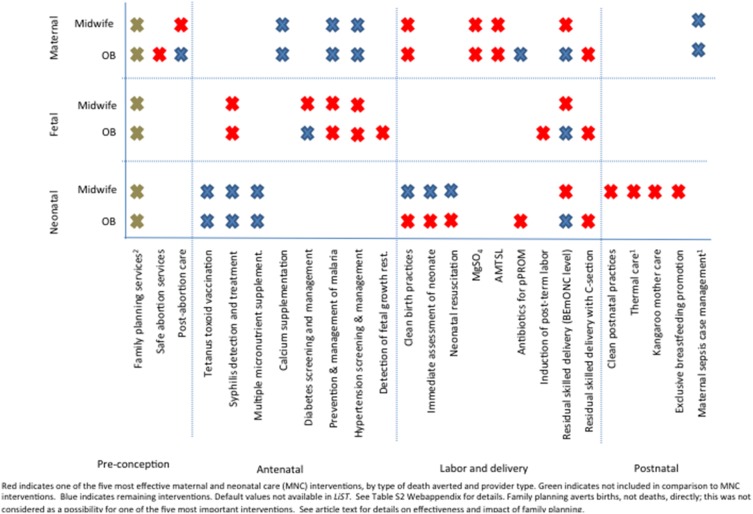
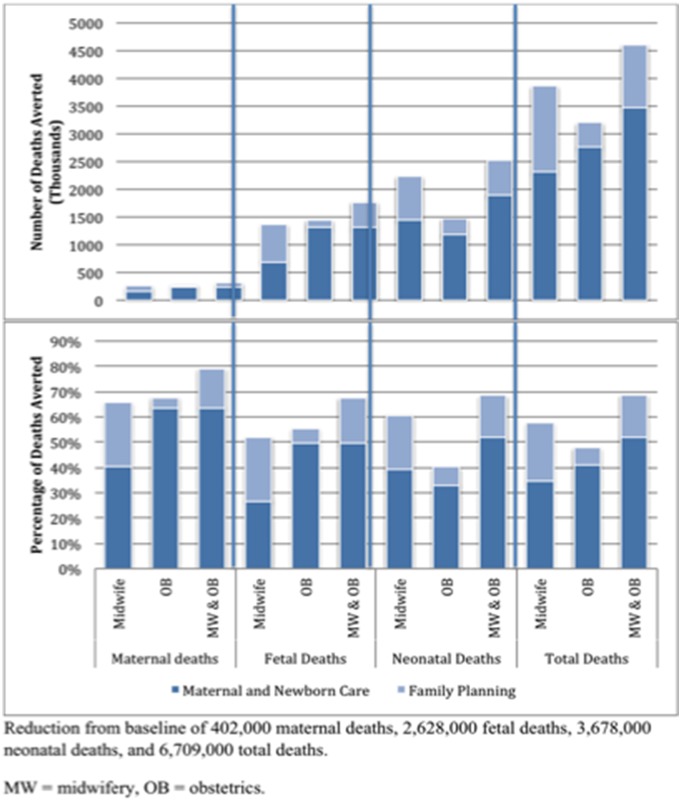
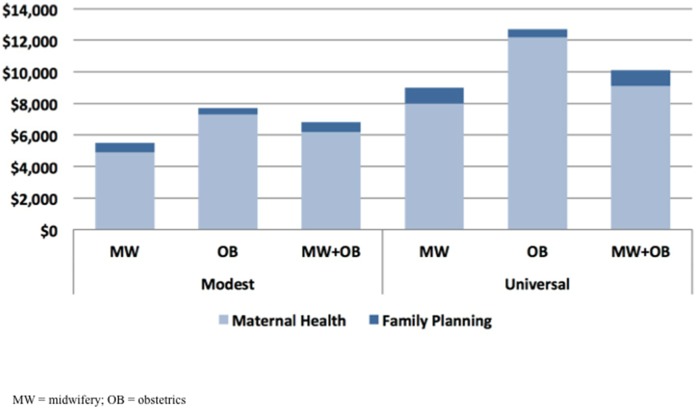
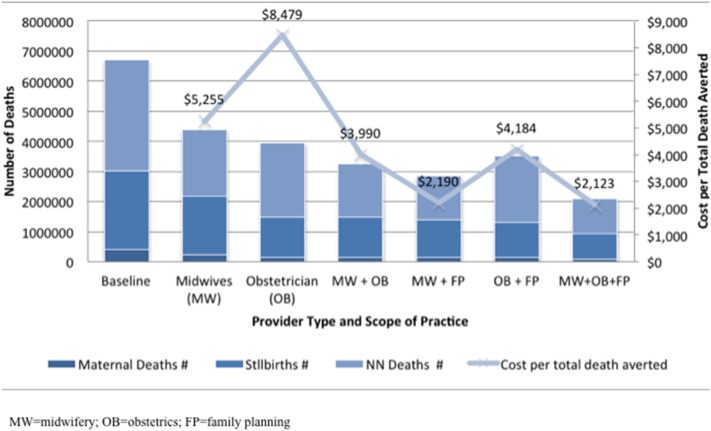
Findings: Under even a modest scale-up, midwifery services including family planning reduce maternal, fetal, and neonatal deaths by 34%. Increasing midwifery alone or integrated with obstetrics is more cost-effective than scaling up obstetrics alone; when family planning was included, the midwifery model was almost twice as cost-effective as the obstetrics model, at $2,200 versus $4,200 per death averted. The most effective strategy was the most comprehensive: increasing midwives, obstetricians, and family planning could prevent 69% of total deaths under universal scale-up, yielding a cost per death prevented of just $2,100. Within this analysis, the interventions which midwifery and obstetrics are poised to deliver most effectively are different, with midwifery benefits delivered across the continuum of pre-pregnancy, prenatal, labor and delivery, and postpartum-postnatal care, and obstetrics benefits focused mostly on delivery. Including family planning within each scope of practice reduced the number of likely births, and thus deaths, and increased the cost-effectiveness of the entire package (e.g., a 52% reduction in deaths with midwifery and obstetrics increased to 69% when family planning was added; cost decreased from $4,000 to $2,100 per death averted).
Conclusions: This analysis suggests that scaling up midwifery and obstetrics could bring many countries closer to achieving mortality reductions. Midwives alone can achieve remarkable mortality reductions, particularly when they also perform family planning services--the greatest return on investment occurs with the scale-up of midwives and obstetricians together.
Conflict of interest statement
Figures
Similar articles
-
Potential impact of midwives in preventing and reducing maternal and neonatal mortality and stillbirths: a Lives Saved Tool modelling study.Lancet Glob Health. 2021 Jan;9(1):e24-e32. doi: 10.1016/S2214-109X(20)30397-1. Epub 2020 Dec 1. Lancet Glob Health. 2021. PMID: 33275948 Free PMC article.
-
The projected effect of scaling up midwifery.Lancet. 2014 Sep 20;384(9948):1146-57. doi: 10.1016/S0140-6736(14)60790-X. Epub 2014 Jun 22. Lancet. 2014. PMID: 24965814 Review.
-
Triple return on investment: the cost and impact of 13 interventions that could prevent stillbirths and save the lives of mothers and babies in South Africa.BMC Pregnancy Childbirth. 2015 Feb 18;15:39. doi: 10.1186/s12884-015-0456-9. BMC Pregnancy Childbirth. 2015. PMID: 25879579 Free PMC article.
-
Measuring the cost-effectiveness of midwife-led versus physician-led intrapartum teams in developing countries.Womens Health (Lond). 2015 Jul;11(4):553-64. doi: 10.2217/WHE.15.18. Epub 2015 Aug 10. Womens Health (Lond). 2015. PMID: 26258663 Review.
-
Alternative strategies to reduce maternal mortality in India: a cost-effectiveness analysis.PLoS Med. 2010 Apr 20;7(4):e1000264. doi: 10.1371/journal.pmed.1000264. PLoS Med. 2010. PMID: 20421922 Free PMC article.
Cited by
-
The effect of increasing the supply of skilled health providers on pregnancy and birth outcomes: evidence from the midwives service scheme in Nigeria.BMC Health Serv Res. 2016 Aug 23;16(1):425. doi: 10.1186/s12913-016-1688-8. BMC Health Serv Res. 2016. PMID: 27613502 Free PMC article.
-
Are there decision support tools that might strengthen the health system for perinatal care in South African district hospitals? A review of the literature.BMC Health Serv Res. 2019 Oct 22;19(1):731. doi: 10.1186/s12913-019-4583-2. BMC Health Serv Res. 2019. PMID: 31640655 Free PMC article. Review.
-
Ninety-one years of midwifery continuity of care in low and middle-income countries: a scoping review.BMC Health Serv Res. 2025 Mar 28;25(1):463. doi: 10.1186/s12913-025-12612-0. BMC Health Serv Res. 2025. PMID: 40155967 Free PMC article.
-
Prevention and Screening for Cardiometabolic Disease Following Hypertensive Disorders in Pregnancy in Low-Resource Settings: A Systematic Review and Delphi Study.Glob Heart. 2023 Apr 25;18(1):21. doi: 10.5334/gh.1195. eCollection 2023. Glob Heart. 2023. PMID: 37125389 Free PMC article.
-
The return of the Traditional Birth Attendant.J Glob Health. 2016 Dec;6(2):020302. doi: 10.7189/jogh.06.020302. J Glob Health. 2016. PMID: 27606054 Free PMC article. No abstract available.
References
-
- United Nations (2012) The Millennium Development Goals Report 2012. New York: United Nations.
-
- World Health Organization, UNICEF (2012) Countdown to 2015: Maternal, Newborn & Child Survival. Building a Future for Women and Children: The 2012 Report. Washington, DC: World Health Organization.
-
- Koblinsky M, Matthews Z, Hussein J, Mavalankar D, Mridha MK, et al. (2006) Going to scale with professional skilled care. Lancet 368: 1377–1386. - PubMed
-
- Graham WJ, Bell JS, Bullough CHW (2001) Can Skilled Attendance at Delivery Reduce Maternal Mortality in Developing Countries? In: Antwerp, Belgium, ITGPress Safe motherhood strategies: a review of the evidence. Vincent De Brouwere, Wim Van Lerberghe, editors. 2001: 97–129 (Studies in Health Services Organisation and Policy No. 17)..
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
