

Veno-venous extracorporeal CO2 removal for the treatment of severe respiratory acidosis: pathophysiological and technical considerations
- PMID: 24942014
- PMCID: PMC4095596
- DOI: 10.1186/cc13928
Veno-venous extracorporeal CO2 removal for the treatment of severe respiratory acidosis: pathophysiological and technical considerations
Abstract
Introduction: While non-invasive ventilation aimed at avoiding intubation has become the modality of choice to treat mild to moderate acute respiratory acidosis, many severely acidotic patients (pH <7.20) still need intubation. Extracorporeal veno-venous CO2 removal (ECCO2R) could prove to be an alternative. The present animal study tested in a systematic fashion technical requirements for successful ECCO2R in terms of cannula size, blood and sweep gas flow.
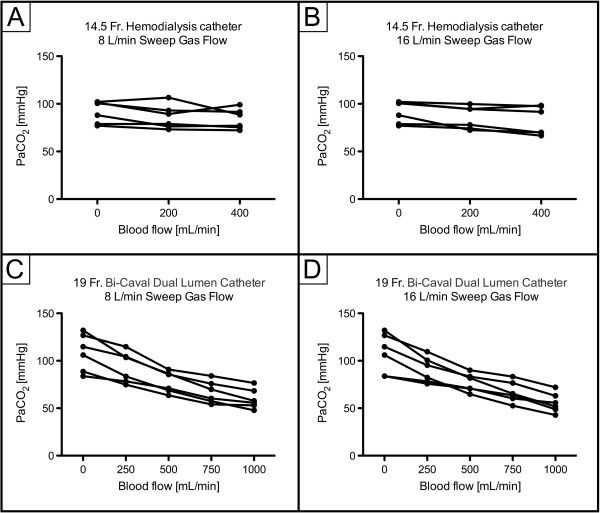
Methods: ECCO2R with a 0.98 m(2) surface oxygenator was performed in six acidotic (pH <7.20) pigs using either a 14.5 French (Fr) or a 19Fr catheter, with sweep gas flow rates of 8 and 16 L/minute, respectively. During each experiment the blood flow was incrementally increased to a maximum of 400 mL/minute (14.5Fr catheter) and 1000 mL/minute (19Fr catheter).
Results: Amelioration of severe respiratory acidosis was only feasible when blood flow rates of 750 to 1000 mL/minute (19Fr catheter) were used. Maximal CO2-elimination was 146.1 ± 22.6 mL/minute, while pH increased from 7.13 ± 0.08 to 7.41 ± 0.07 (blood flow of 1000 mL/minute; sweep gas flow 16 L/minute). Accordingly, a sweep gas flow of 8 L/minute resulted in a maximal CO2-elimination rate of 138.0 ± 16.9 mL/minute. The 14.5Fr catheter allowed a maximum CO2 elimination rate of 77.9 mL/minute, which did not result in the normalization of pH.
Conclusions: Veno-venous ECCO2R may serve as a treatment option for severe respiratory acidosis. In this porcine model, ECCO2R was most effective when using blood flow rates ranging between 750 and 1000 mL/minute, while an increase in sweep gas flow from 8 to 16 L/minute had less impact on ECCO2R in this setting.
Figures





Comment in
-
Veno-venous extracorporeal CO2 removal for the treatment of severe respiratory acidosis.Crit Care. 2015 Apr 17;19(1):176. doi: 10.1186/s13054-015-0769-0. Crit Care. 2015. PMID: 25927222 Free PMC article. No abstract available.
References
-
- Hoo GW, Hakimian N, Santiago SM. Hypercapnic respiratory failure in COPD patients: response to therapy. Chest. 2000;117:169–177. - PubMed
-
- Quinnell TG, Pilsworth S, Shneerson JM, Smith IE. Prolonged invasive ventilation following acute ventilatory failure in COPD: weaning results, survival, and the role of noninvasive ventilation. Chest. 2006;129:133–139. - PubMed
-
- Ambrosino N, Vagheggini G. Noninvasive positive pressure ventilation in the acute care setting: where are we? Eur Respir J. 2008;31:874–886. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
