

Diagnostic accuracy of quantitative PCR (Xpert MTB/RIF) for tuberculous pericarditis compared to adenosine deaminase and unstimulated interferon-γ in a high burden setting: a prospective study
- PMID: 24942470
- PMCID: PMC4073812
- DOI: 10.1186/1741-7015-12-101
Diagnostic accuracy of quantitative PCR (Xpert MTB/RIF) for tuberculous pericarditis compared to adenosine deaminase and unstimulated interferon-γ in a high burden setting: a prospective study
Abstract
Background: Tuberculous pericarditis (TBP) is associated with high morbidity and mortality, and is an important treatable cause of heart failure in developing countries. Tuberculous aetiology of pericarditis is difficult to diagnose promptly. The utility of the new quantitative PCR test (Xpert MTB/RIF) for the diagnosis of TBP is unknown. This study sought to evaluate the diagnostic accuracy of the Xpert MTB/RIF test compared to pericardial adenosine deaminase (ADA) and unstimulated interferon-gamma (uIFNγ) in suspected TBP.
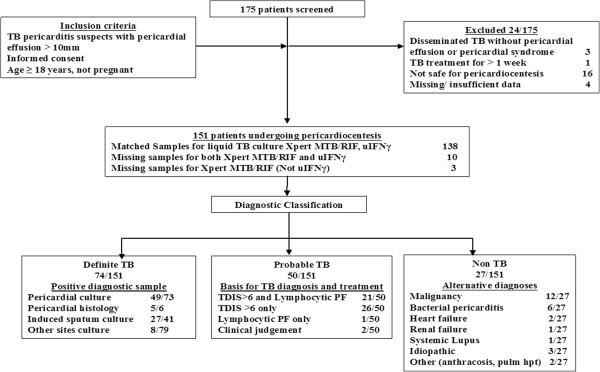
Methods: From October 2009 through September 2012, 151 consecutive patients with suspected TBP were enrolled at a single centre in Cape Town, South Africa. Mycobacterium tuberculosis culture and/or pericardial histology served as the reference standard for definite TBP. Receiver-operating-characteristic curve analysis was used for selection of ADA and uIFNγ cut-points.
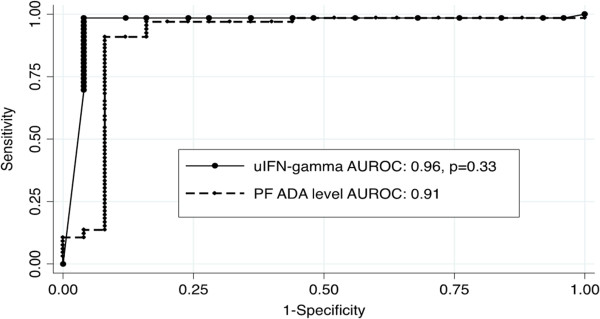
Results: Of the participants, 49% (74/151) were classified as definite TBP, 33% (50/151) as probable TBP and 18% (27/151) as non TBP. A total of 105 (74%) participants were human immunodeficiency virus (HIV) positive. Xpert-MTB/RIF had a sensitivity and specificity (95% confidence interval (CI)) of 63.8% (52.4% to 75.1%) and 100% (85.6% to 100%), respectively. Concentration of pericardial fluid by centrifugation and using standard sample processing did not improve Xpert MTB/RIF accuracy. ADA (≥35 IU/L) and uIFNγ (≥44 pg/ml) both had a sensitivity of 95.7% (88.1% to 98.5%) and a negative likelihood ratio of 0.05 (0.02 to 0.10). However, the specificity and positive likelihood ratio of uIFNγ was higher than ADA (96.3% (81.7% to 99.3%) and 25.8 (3.6 to 183.4) versus 84% (65.4% to 93.6%) and 6.0 (3.7 to 9.8); P = 0.03) at an estimated background prevalence of TB of 30%. The sensitivity and negative predictive value of both uIFNγ and ADA were higher than Xpert-MT/RIF (P < 0.001).
Conclusions: uIFNγ offers superior accuracy for the diagnosis of microbiologically confirmed TBP compared to the ADA assay and the Xpert MTB/RIF test.
Figures
References
-
- World Health Organization. Global Tuberculosis Report 2013. Geneva; 2013.
-
- Maartens G, Wilkinson RJ. Tuberculosis. Lancet. 2007;370:2030–2043. - PubMed
-
- Mayosi BM, Wiysonge CS, Ntsekhe M, Volmink JA, Gumedze F, Maartens G, Aje A, Thomas BM, Thomas KM, Awotedu AA, Thembela B, Mntla P, Maritz F, Blackett KN, Nkouonlack DC, Burch VC, Rebe K, Parrish A, Sliwa K, Vezi BZ, Alam N, Brown BG, Gould T, Visser T, Magula NP, Commerford PJ. Mortality in patients treated for tuberculous pericarditis in sub-Saharan Africa. S Afr Med J. 2008;98:36–40. - PubMed
-
- Damasceno A, Mayosi BM, Sani M, Ogah OS, Mondo C, Dike O, Dzudie A, Kouam Kouam C, Suliman A, Schrueder N, Yonga G, Ba SA, Maru F, Alemayehu B, Edwards C, Davison BA, Cotter G, Sliwa K. The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries: results of the sub-saharan africa survey of heart failure. Arch Int Med. 2012;172:1386–1394. - PubMed
-
- Mayosi BM, Burgess LJ, Doubell AF. Tuberculous pericarditis. Circulation. 2005;112:3608–3616. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
