

Developing a reference of normal lung sounds in healthy Peruvian children
- PMID: 24943262
- PMCID: PMC5983893
- DOI: 10.1007/s00408-014-9608-3
Developing a reference of normal lung sounds in healthy Peruvian children
Abstract
Purpose: Lung auscultation has long been a standard of care for the diagnosis of respiratory diseases. Recent advances in electronic auscultation and signal processing have yet to find clinical acceptance; however, computerized lung sound analysis may be ideal for pediatric populations in settings, where skilled healthcare providers are commonly unavailable. We described features of normal lung sounds in young children using a novel signal processing approach to lay a foundation for identifying pathologic respiratory sounds.
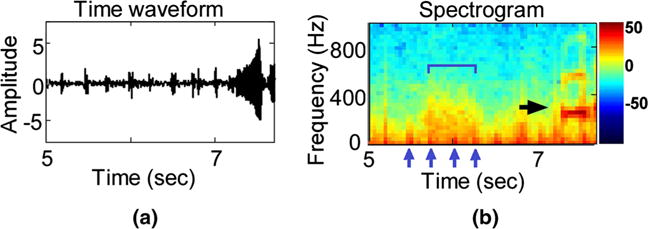
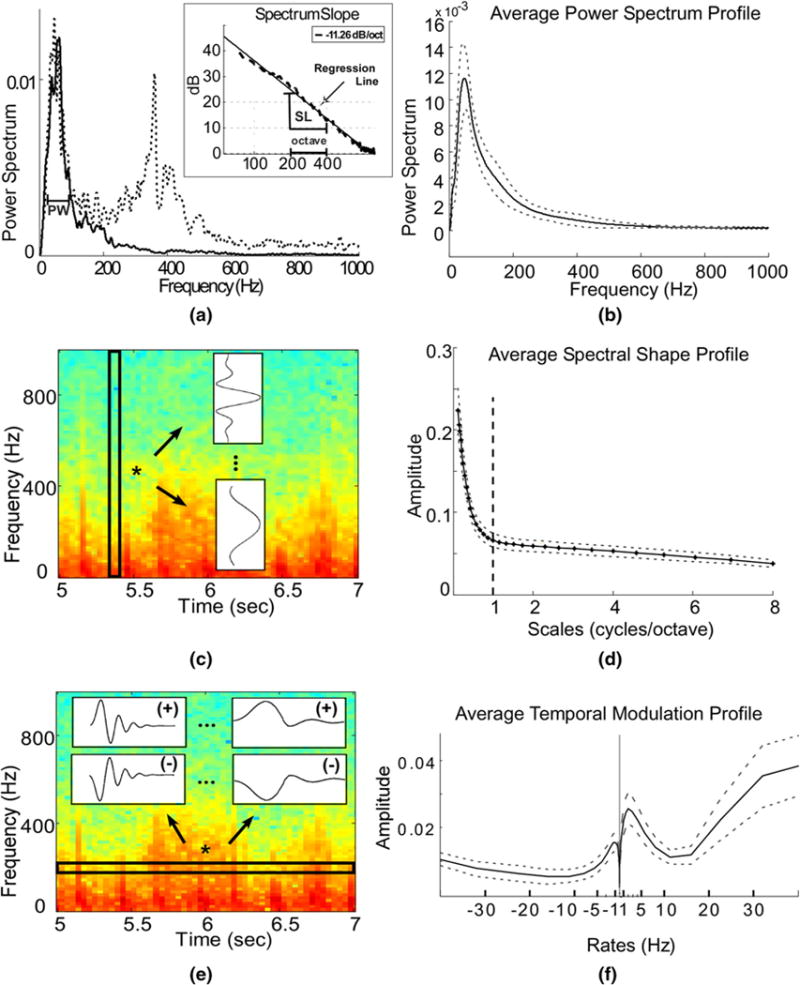
Methods: 186 healthy children with normal pulmonary exams and without respiratory complaints were enrolled at a tertiary care hospital in Lima, Peru. Lung sounds were recorded at eight thoracic sites using a digital stethoscope. 151 (81%) of the recordings were eligible for further analysis. Heavy-crying segments were automatically rejected and features extracted from spectral and temporal signal representations contributed to profiling of lung sounds.
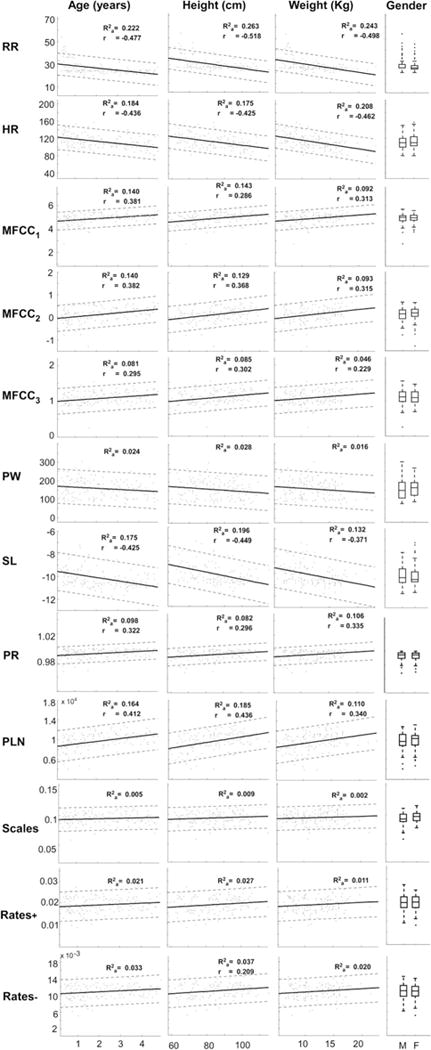
Results: Mean age, height, and weight among study participants were 2.2 years (SD 1.4), 84.7 cm (SD 13.2), and 12.0 kg (SD 3.6), respectively; and, 47% were boys. We identified ten distinct spectral and spectro-temporal signal parameters and most demonstrated linear relationships with age, height, and weight, while no differences with genders were noted. Older children had a faster decaying spectrum than younger ones. Features like spectral peak width, lower-frequency Mel-frequency cepstral coefficients, and spectro-temporal modulations also showed variations with recording site.
Conclusions: Lung sound extracted features varied significantly with child characteristics and lung site. A comparison with adult studies revealed differences in the extracted features for children. While sound-reduction techniques will improve analysis, we offer a novel, reproducible tool for sound analysis in real-world environments.
Conflict of interest statement
All authors in the study report no conflict of interest.
Figures
References
-
- Grenier MC, Gagnon K, Genest J, Jr, Durand J, Durand LG. Clinical comparison of acoustic and electronic stethoscopes and design of a new electronic stethoscope. Am J Cardiol. 1998;81:653–656. - PubMed
-
- Guntupalli KK, Alapat PM, Bandi VD, Kushnir I. Validation of automatic wheeze detection in patients with obstructed airways and in healthy subjects. J Asthma. 2008;45:903–907. - PubMed
-
- Murphy RL, Vyshedskiy A, Power-Charnitsky VA, Bana DS, Marinelli PM, Wong-Tse A, Paciej R. Automated lung sound analysis in patients with pneumonia. Respir Care. 2004;49:1490–1497. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
