

The cost effectiveness of a tailored, web-based care program to enhance postoperative recovery in gynecologic patients in comparison with usual care: protocol of a stepped wedge cluster randomized controlled trial
- PMID: 24943277
- PMCID: PMC4090379
- DOI: 10.2196/resprot.3236
The cost effectiveness of a tailored, web-based care program to enhance postoperative recovery in gynecologic patients in comparison with usual care: protocol of a stepped wedge cluster randomized controlled trial
Abstract
Background: The length of recovery after benign gynecological surgery and return to work frequently exceeds the period that is recommended or expected by specialists. A prolonged recovery is associated with a poorer quality of life. In addition, costs due to prolonged sick leave following gynecological surgery cause a significant financial burden on society.
Objective: The objective of our study was to present the protocol of a stepped wedge cluster randomized controlled trial to evaluate the cost effectiveness of a new care program for patients undergoing hysterectomy and/or adnexal surgery for benign disease, compared to the usual care.
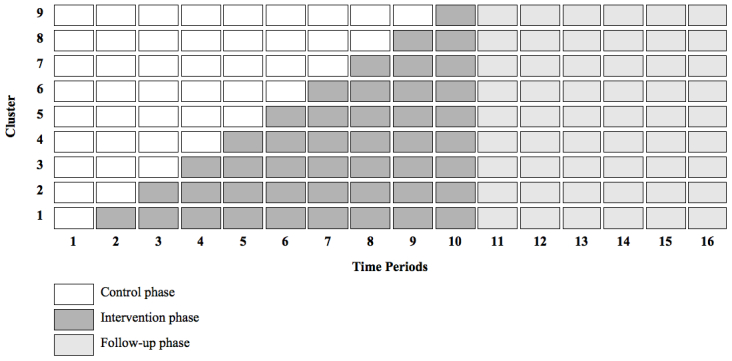
Methods: The care program under study, designed to improve convalescence and to prevent delayed return to work, targets two levels. At the hospital level, guidelines will be distributed among clinical staff in order to stimulate evidence-based patient education. At the patient level, additional perioperative guidance is provided by means of an eHealth intervention, equipping patients with tailored convalescence advice, and an occupational intervention is available for those patients at risk of prolonged sick leave. Due to the stepped wedge design of the trial, the care program will be sequentially rolled out among the 9 participating hospitals, from which the patients are recruited. Eligible for this study are employed women, 18-65 years of age, who are scheduled for hysterectomy and/or laparoscopic adnexal surgery. The primary outcome is full sustainable return to work. The secondary outcomes include general recovery, quality of life, self-efficacy, coping, and pain. The data will be collected by means of self-reported electronic questionnaires before surgery and at 2, 6, 12, 26, and 52 weeks after surgery. Sick leave and cost data are measured by monthly sick leave calendars, and cost diaries during the 12 month follow-up period. The economic evaluation will be performed from the societal perspective. All statistical analyses will be conducted according to the intention-to-treat principle.
Results: The enrollment of the patients started October 2011. The follow-up period will be completed in August 2014. Data cleaning or analysis has not begun as of this article's submission.
Conclusions: We hypothesize the care program to be effective by means of improving convalescence and reducing costs associated with productivity losses following gynecological surgery. The results of this study will enable health care policy makers to decide about future implementation of this care program on a broad scale.
Trial registration: Netherlands Trial Register: NTR2933; http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=2933 (Archived by WebCite at http://www.webcitation.org/6Q7exPG84).
Keywords: Internet; convalescence; economic evaluation; gynecology; return to work; telemedicine.
Conflict of interest statement
Conflicts of Interest: EVB, AVN, HAB, JRA, and JAH are the developers of the care program under study.
Figures

References
-
- Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg. 2002 Jun;183(6):630–641. - PubMed
-
- Kjølhede P, Borendal Wodlin N, Nilsson L, Fredrikson M, Wijma K. Impact of stress coping capacity on recovery from abdominal hysterectomy in a fast-track programme: A prospective longitudinal study. BJOG. 2012 Jul;119(8):998–1006; discussion 1006. doi: 10.1111/j.1471-0528.2012.03342.x. - DOI - PubMed
-
- Horvath KJ. Postoperative recovery at home after ambulatory gynecologic laparoscopic surgery. J Perianesth Nurs. 2003 Oct;18(5):324–334. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
