

Classical Renin-Angiotensin system in kidney physiology
- PMID: 24944035
- PMCID: PMC4137912
- DOI: 10.1002/cphy.c130040
Classical Renin-Angiotensin system in kidney physiology
Abstract
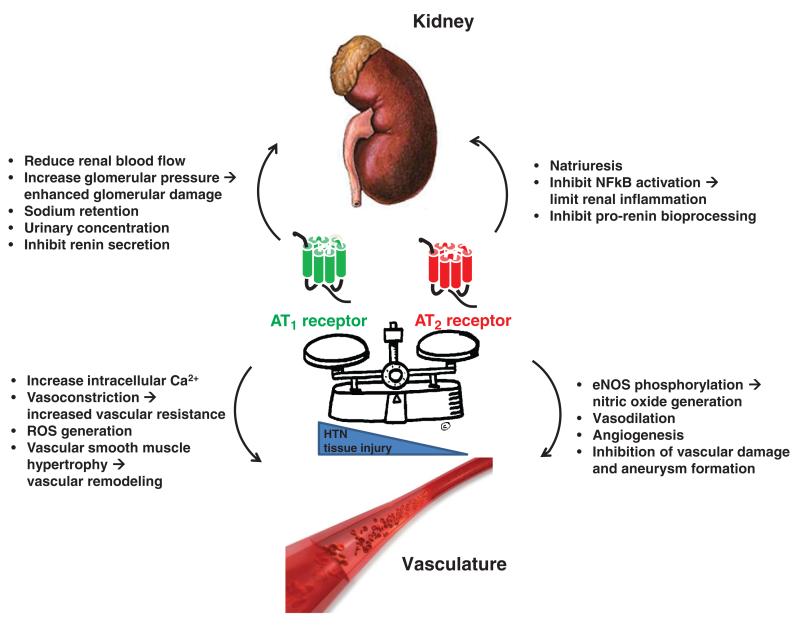
The renin-angiotensin system has powerful effects in control of the blood pressure and sodium homeostasis. These actions are coordinated through integrated actions in the kidney, cardiovascular system and the central nervous system. Along with its impact on blood pressure, the renin-angiotensin system also influences a range of processes from inflammation and immune responses to longevity. Here, we review the actions of the "classical" renin-angiotensin system, whereby the substrate protein angiotensinogen is processed in a two-step reaction by renin and angiotensin converting enzyme, resulting in the sequential generation of angiotensin I and angiotensin II, the major biologically active renin-angiotensin system peptide, which exerts its actions via type 1 and type 2 angiotensin receptors. In recent years, several new enzymes, peptides, and receptors related to the renin-angiotensin system have been identified, manifesting a complexity that was previously unappreciated. While the functions of these alternative pathways will be reviewed elsewhere in this journal, our focus here is on the physiological role of components of the "classical" renin-angiotensin system, with an emphasis on new developments and modern concepts.
© 2014 American Physiological Society.
Figures









References
-
- Allen AM, Dosanjh JK, Erac M, Dassanayake S, Hannan RD, Thomas WG. Expression of constitutively active angiotensin receptors in the rostral ventrolateral medulla increases blood pressure. Hypertension. 2006;47:1054–1061. - PubMed
-
- Amlal H, LeGoff C, Vernimmen C, Soleimani M, Paillard M, Bichara M. ANG II controls Na(+)-K (NH4)-2Cl-cotransport via 20-HETE and PKC in medullary thick ascending + +limb. Am J Physiol. 1998;274:C1047–C1056. - PubMed
-
- Andresen BT, Romero GG, Jackson EK. AT2 receptors attenuate AT1 receptor-induced phospholipase D activation in vascular smooth muscle cells. J Pharmacol Exp Ther. 2004;309:425–431. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
