

Clinicopathological findings in a case series of abdominopelvic solitary fibrous tumors
- PMID: 24944670
- PMCID: PMC3961353
- DOI: 10.3892/ol.2014.1872
Clinicopathological findings in a case series of abdominopelvic solitary fibrous tumors
Abstract
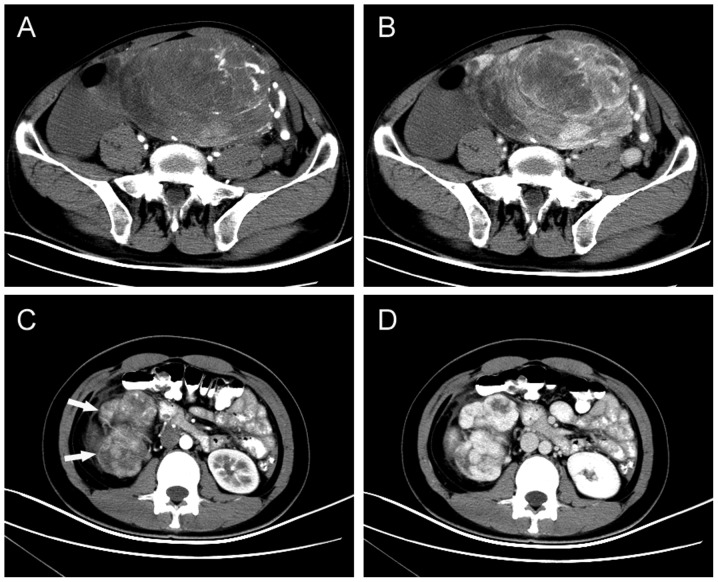
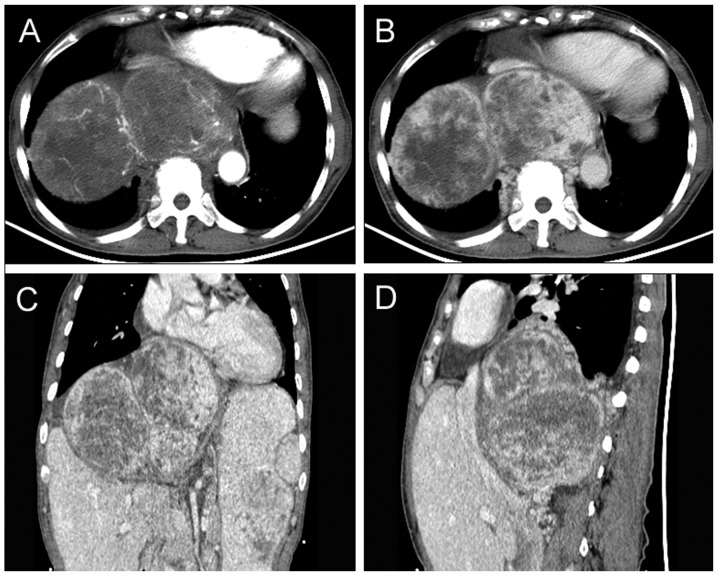
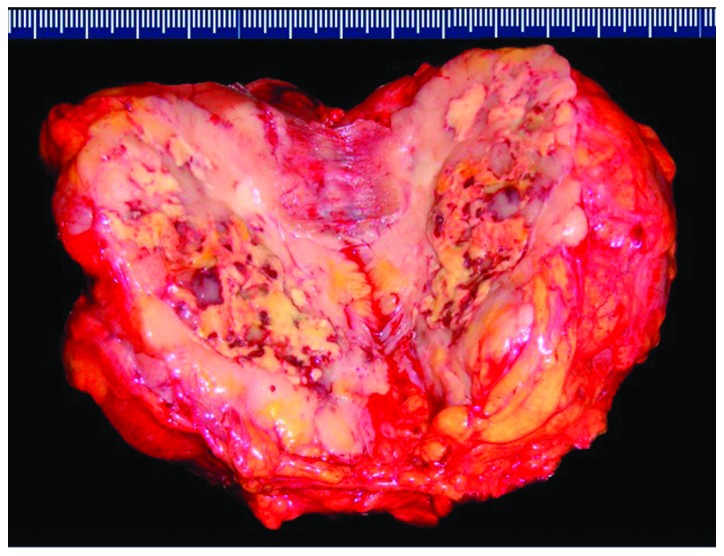
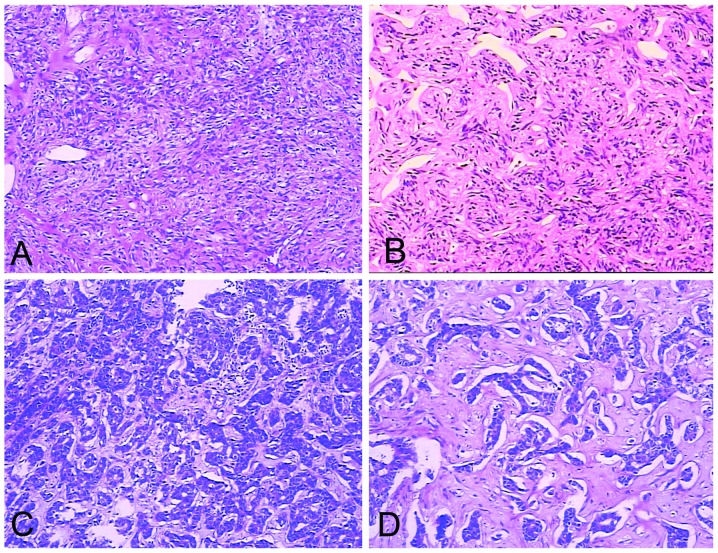
Solitary fibrous tumors (SFTs) represent a rare type of soft tissue tumor. Extrathoracic SFTs (ESFTs) in the soft tissues of the abdominopelvic cavity are extremely rare. Between January 2002 and January 2013, 10 patients were identified with abdominopelvic SFTs at the Northern Jiangsu People's Hospital. The clinicopathological data, treatment and follow-up results were retrospectively analyzed in this study. Patients included four females and six males, whose age ranged between 21 and 75 years (mean, 53.3 years). The maximum diameter of the tumors was 2.5-28 cm (mean, 12.7 cm). Two cases were diagnosed as malignant variants of ESFTs. R0 resection was performed in eight patients, while one patient underwent R1 resection, and one patient received palliative chemotherapy for an inoperable mass. Follow-up time ranged between 6 and 126 months (mean, 50 months). The patient with R1 resection suffered a local relapse, and the patient receiving palliative chemotherapy succumbed to the disease. The remaining eight patients remained free of disease. Abdominopelvic SFTs usually reveal an indolent process, although the majority of tumors in the present study were of giant size when diagnosed. The risk of local recurrence and metastasis correlates with tumor size and the histological status of surgical margins. The preferred treatment is complete resection followed by extended follow-up surveillance.
Keywords: histopathology; immunohistochemistry; solitary fibrous tumor; spindle cell tumor.
Figures
References
-
- Klemperer P, Rabin CB. Primary neoplasmas of the pleura. A report of five cases. Am J Ind Med. 1992;22:4–31. - PubMed
-
- Gold JS, Antonescu CR, Hajdu C, et al. Clinicopathologic correlates of solitary fibrous tumors. Cancer. 2002;94:1057–1068. - PubMed
-
- Brunnemann RB, Ro JY, Ordonez NG, Mooney J, El-Naggar AK, Ayala AG. Extrapleural solitary fibrous tumor: a clinicopathologic study of 24 cases. Mod Pathol. 1999;12:1034–1042. - PubMed
-
- Fukunaga M, Naganuma H, Nikaido T, Harada T, Ushigome S. Extrapleural solitary fibrous tumor: a report of seven cases. Mod Pathol. 1997;10:443–450. - PubMed
-
- Hasegawa T, Matsuno Y, Shimoda T, Hasegawa F, Sano T, Hirohashi S. Extrathoracic solitary fibrous tumors: their histological variability and potentially aggressive behavior. Hum Pathol. 1999;30:1464–1473. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources