

Diagnosis of Pathologically Early HCC with EOB-MRI: Experiences and Current Consensus
- PMID: 24945000
- PMCID: PMC4057792
- DOI: 10.1159/000343865
Diagnosis of Pathologically Early HCC with EOB-MRI: Experiences and Current Consensus
Abstract
Objective: After much debate, the International Consensus Group for Hepatocellular Neoplasia (ICGHN) has recently arrived at a conclusion regarding the pathological criteria for early hepatocellular carcinoma (HCC). They have stated that stromal invasion should be recognized as the most important pathological finding for precisely diagnosing and differentiating early HCC from dysplastic nodules (DN).
Methods: We conducted a review of the imaging findings from multi-imaging modalities of early HCC cases diagnosed according to the pathological criteria of the ICGHN. The multi-imaging modalities included gadoxetic acid (Gd-EOB-DTPA) enhanced magnetic resonance imaging (MRI), abbreviated as EOB-MRI, contrast-enhanced CT (CE-CT), CT during arterioportography (CTAP), and CT during hepatic arteriography (CTHA). It has been shown that EOB-MRI is the only imaging modality that has sufficient resolution for the detection and classification of early HCC.
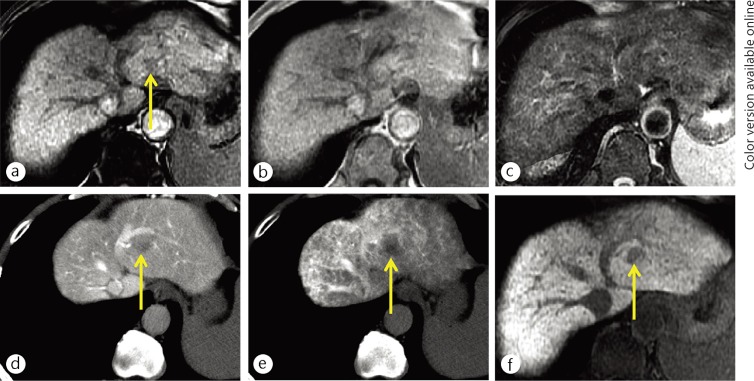
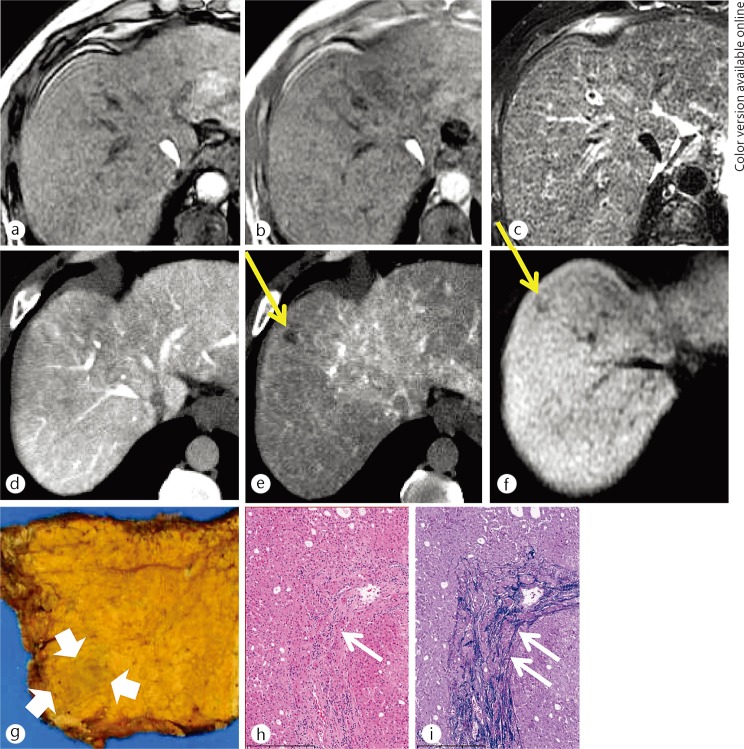
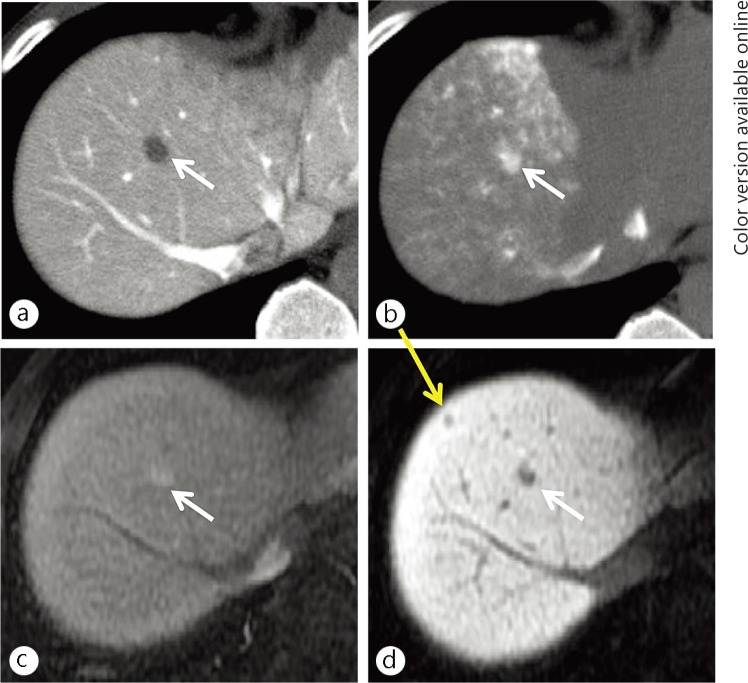
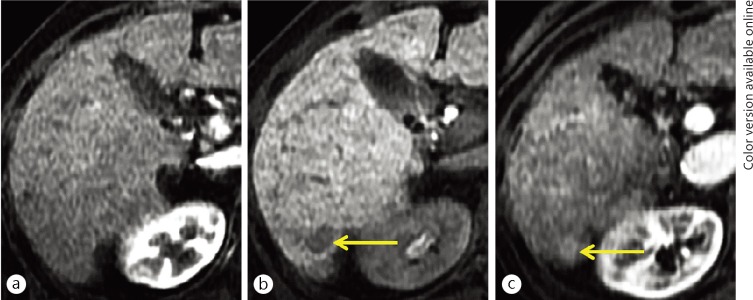
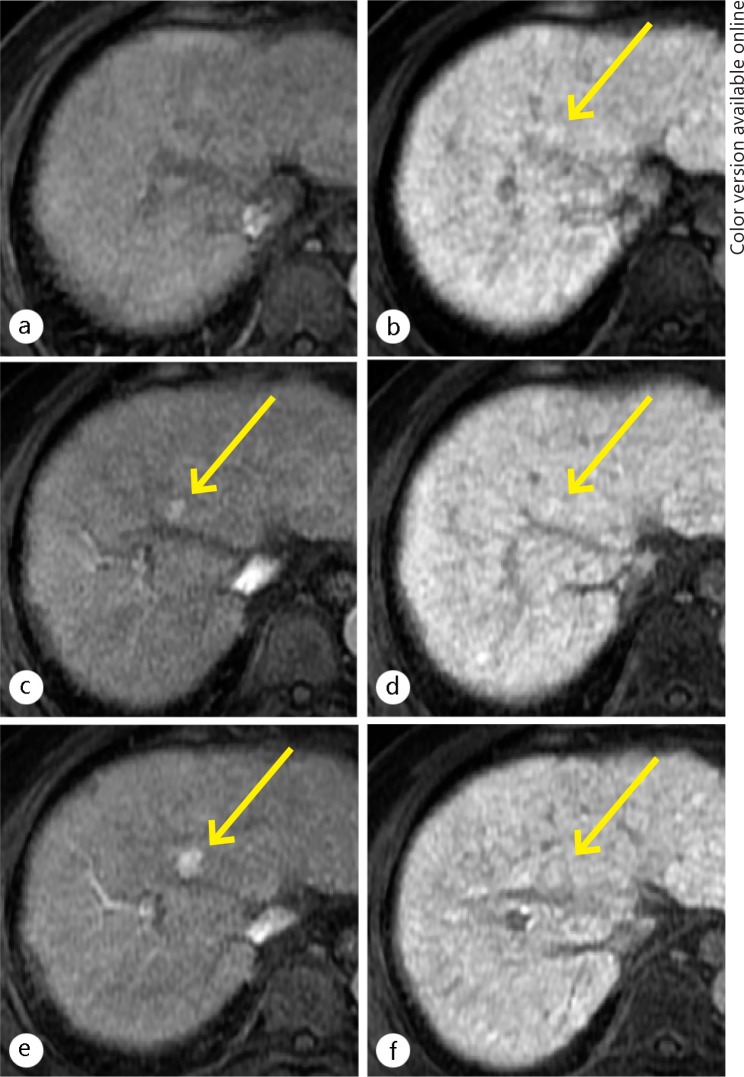
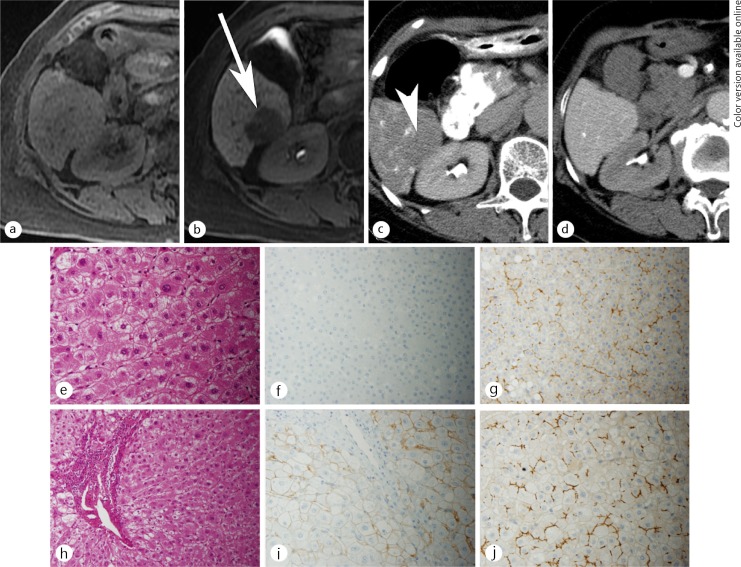
Results: The most significant imaging feature for diagnosing early HCC was hypointensity on hepatobiliary-phase (HP) images of EOB-MRI; all of the cases of early HCC that were detected on HP images of EOB-MRI showed hypointensity, while all of the images of DN showed isointensity or hyperintensity compared with the liver parenchyma. The results of the diagnostic performance analysis showed that EOB-MRI had excellent sensitivity (97%) for detecting early HCC and outstanding specificity (100%) for distinguishing early HCC from DN.
Conclusions: Considering the results from imaging-pathologic correlations and follow-up studies indicating that many early-stage hepatocellular nodules showing hypointensity on HP images of EOB-MRI tend to develop hypervascularization during a relatively short follow-up period, it is beginning to be accepted that such nodules may be treated as early HCC. However, hepatologists and radiologists should also recognize that some cases of early HCC may show isointensity or hyperintensity on HP images of EOB-MRI, making it impossible to differentiate early HCC from DN, although the low prevalence of such nodules may be unlikely to affect the generally accepted follow-up protocols for cirrhotic patients. Our results and other recent reports have indicated that signal-intensity patterns on HP images of EOB-MRI for DN and early HCC directly correlate with the degree of expression of the organic anion transporting polypeptide (OATP) 1B3 in the nodules. Thus, the diagnostic performance of pathological analyses for early HCC cases may be dramatically improved, nearly up to that of EOB-MRI, by incorporating an OATP1B3 staining method.
Keywords: Early hepatocellular carcinoma; Gadoxetic acid; MRI; OATP1B3.
Figures
References
-
- Kudo M. Multistep human hepatocarcinogenesis: correlation of imaging with pathology. J Gastroenterol. 2009;44(Suppl 19):112–118. - PubMed
-
- Kitao A, Zen Y, Matsui O, Gabata T, Nakanuma Y. Hepatocarcinogenesis: multistep changes of drainage vessels at CT during arterial portography and hepatic arteriography—radiologic-pathologic correlation. Radiology. 2009;252:605–614. - PubMed
-
- Sakamoto M, Hirohashi S, Shimosato Y. Early stages of multistep hepatocarcinogenesis: adenomatous hyperplasia and early hepatocellular carcinoma. Hum Pathol. 1991;22:172–178. - PubMed
-
- International Working Party Terminology of nodular hepatocellular lesions. Hepatology. 1995;22:983–993. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
