

Prediction of acute respiratory disease in current and former smokers with and without COPD
- PMID: 24945159
- PMCID: PMC4188150
- DOI: 10.1378/chest.13-2946
Prediction of acute respiratory disease in current and former smokers with and without COPD
Abstract
Background: The risk factors for acute episodes of respiratory disease in current and former smokers who do not have COPD are unknown.
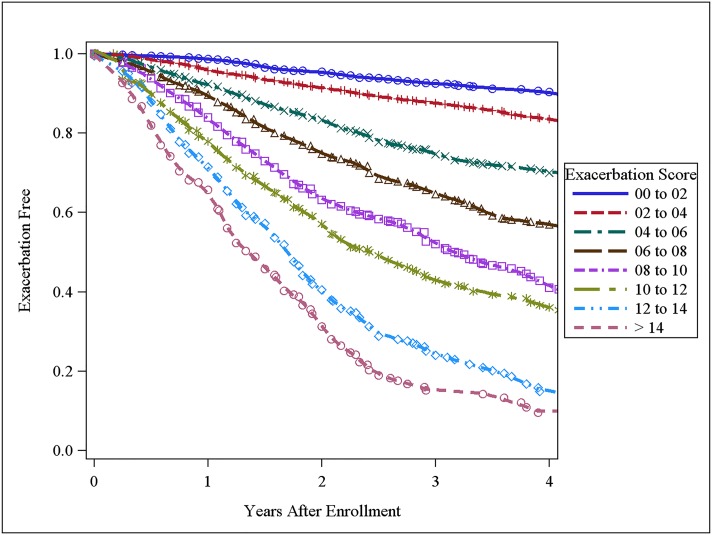
Methods: Eight thousand two hundred forty-six non-Hispanic white and black current and former smokers in the Genetic Epidemiology of COPD (COPDGene) cohort had longitudinal follow-up (LFU) every 6 months to determine acute respiratory episodes requiring antibiotics or systemic corticosteroids, an ED visit, or hospitalization. Negative binomial regression was used to determine the factors associated with acute respiratory episodes. A Cox proportional hazards model was used to determine adjusted hazard ratios (HRs) for time to first episode and an acute episode of respiratory disease risk score.
Results: At enrollment, 4,442 subjects did not have COPD, 658 had mild COPD, and 3,146 had moderate or worse COPD. Nine thousand three hundred three acute episodes of respiratory disease and 2,707 hospitalizations were reported in LFU (3,044 acute episodes of respiratory disease and 827 hospitalizations in those without COPD). Major predictors included acute episodes of respiratory disease in year prior to enrollment (HR, 1.20; 95% CI, 1.15-1.24 per exacerbation), airflow obstruction (HR, 0.94; 95% CI, 0.91-0.96 per 10% change in % predicted FEV1), and poor health-related quality of life (HR, 1.07; 95% CI, 1.06-1.08 for each 4-unit increase in St. George's Respiratory Questionnaire score). Risks were similar for those with and without COPD.
Conclusions: Although acute episode of respiratory disease rates are higher in subjects with COPD, risk factors are similar, and at a population level, there are more episodes in smokers without COPD.
Figures
References
-
- Ford ES, Mannino DM, Wheaton AG, Giles WH, Presley-Cantrell L, Croft JB. Trends in the prevalence of obstructive and restrictive lung function among adults in the United States: findings from the National Health and Nutrition Examination surveys from 1988-1994 to 2007-2010. Chest. 2013;143(5):1395-1406 - PMC - PubMed
-
- Global strategy for diagnosis, management and prevention of COPD. Global Initiative for Chronic Obstructive Lung Disease website. http://www.goldcopd.com. Accessed September 6, 2013
-
- Strassels SA, Smith DH, Sullivan SD, Mahajan PS. The costs of treating COPD in the United States. Chest. 2001;119(2):344-352 - PubMed
-
- Smucny J, Fahey T, Becker L, Glazier R. Antibiotics for acute bronchitis. Cochrane Database Syst Rev. 2004;(4):CD000245. - PubMed
-
- Anzueto A, Miravitlles M, Ewig S, Legnani D, Heldner S, Stauch K. Identifying patients at risk of late recovery (≥ 8 days) from acute exacerbation of chronic bronchitis and COPD. Respir Med. 2012;106(9):1258-1267 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
