

High prevalence of esophageal dysmotility in asymptomatic obese patients
- PMID: 24945185
- PMCID: PMC4072232
- DOI: 10.1155/2014/960520
High prevalence of esophageal dysmotility in asymptomatic obese patients
Abstract
Background: Obesity is an important health problem affecting >500 million people worldwide. Esophageal dysmotility is a gastrointestinal pathology associated with obesity; however, its prevalence and characteristics remain unclear. Esophageal dysmotilities have a high prevalence among obese patients regardless of gastrointestinal symptoms.
Objective: To identify the prevalence of esophageal dysmotility among obese patients. The secondary goals were to characterize these pathologies in obese patients and identify risk factors.
Method: A prospective study from January 2009 to March 2010 at the University of Montreal Hospital Centre (Montreal, Quebec) was performed. Every patient scheduled for bariatric surgery underwent preoperatory esophageal manometry and was included in the study. Manometry was performed according to a standardized protocol with the following measures: superior esophageal sphincter - coordination and release during deglutition; esophageal body - presence, propagation, length, amplitude and type of esophageal waves of contraction; lower esophageal sphincter - localization, tone, release, intragastic pressure and intraesophageal pressure. All reference values were those used in the digestive motility laboratory. A gastrointestinal symptoms questionnaire was completed on the day manometry was performed. Chart reviews were performed to identify comorbidities and treatments that could influence the results.
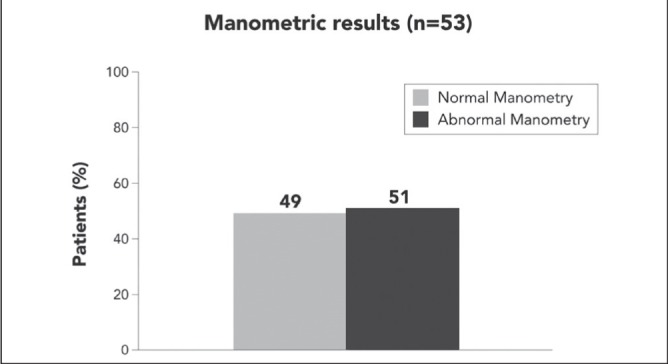
Results: A total of 53 patients were included (mean [± SD] age 43 ± 10 years; mean body mass index 46 ± 7 kg/m; 70% female). Esophageal manometry revealed dysmotility in 51% (n=27) of the patients. This dysmotility involved the esophageal body in 74% (n=20) of the patients and the inferior sphincter in 11% (n=3). Mixed dysmotility (body and inferior sphincter) was found in 15% (n=4) of cases. The esophageal body dysmotilities were hypomotility in 85% (n=23) of the patients, either from insignificant waves (74% [n=20]), nonpropagated waves (11% [n=3]) or low-amplitude waves (33% [n=9]). Gastroesophageal symptoms were found in 66% (n=35) of obese patients, including heartburn (66% [n=23]), regurgitation (26% [n=9]), dysphagia (43% [n=15]), chest pain (6% [n=2]) and dyspepsia (26% [n=9]). Among symptomatic patients, 51% (n=18) had normal manometry and 49% (n=17) had abnormal manometry (statistically nonsignificant). Among asymptomatic patients (n=18), 44% (n=8) had normal manometry and 56% (n=10) had abnormal manometry (statistically nonsignificant). Furthermore, no statistical differences were found between the normal manometry group and the abnormal manometry group with regard to medication intake or comorbidities.
Conclusion: Esophageal dysmotilities had a high prevalence in obese patients. Gastrointestinal symptoms cannot predict the presence of esophageal dysmotility. Hypomotility of the esophageal body is the most common dysmotility, especially from the absence of significant waves.
HISTORIQUE :: L’obésité est un problème de santé important qui touche plus de 500 millions de personnes dans le monde. La dysmotilité œsophagienne est une pathologie gastro-intestinale associée à l’obésité, mais on n’en connaît pas encore la prévalence et les caractéristiques exactes. La prévalence est élevée chez les patients obèses, quels que soient leurs symptômes gastro-intestinaux.
OBJECTIF :: Déterminer la prévalence de dysmotilité œsophagienne chez les patients obèses. Les objectifs secondaires consistaient à caractériser ces pathologies chez les patients obèses et à établir leurs facteurs de risque.
MÉTHODOLOGIE :: Les chercheurs ont mené une étude prospective de janvier 2009 à mars 2010 au Centre hospitalier de l’Université de Montréal, au Québec. Chaque patient devant subir une chirurgie bariatrique s’est soumis à une manométrie œsophagienne préopératoire et a été inclus dans l’étude. La manométrie a été effectuée selon un protocole standardisé faisant appel aux mesures suivantes : le sphincter œsophagien supérieur (coordination et relâchement pendant la déglutition), le corps de l’œsophage (présence, propagation, longueur, amplitude et type d’ondes de contraction de l’œsophage), sphincter inférieur de l’œsophage (emplacement, tonus, relâchement, pression intragastrique et pression intra- œsophagienne). Toutes les valeurs de référence sont celles utilisées au laboratoire de motilité digestive. Les patients ont rempli un questionnaire sur les symptômes gastro-intestinaux le jour de la manométrie. Les chercheurs ont examiné les dossiers pour déterminer les comorbidités et les traitements susceptibles d’influer sur les résultats.
RÉSULTATS :: Au total, 53 patients ont participé à l’étude (âge moyen [±ÉT] de 43±10 ans; indice de masse corporelle moyen de 46±7 kg/m2; 70 % de femmes). La manométrie de l’œsophage a révélé une dysmotilité chez 51 % (n=27) des patients. Cette dysmotilité touchait le corps de l’œsophage chez 74 % des patients (n=20) et le sphincter inférieur chez 11 % d’entre eux (n=3). Une dysmotilité mixte (corps et sphincter inférieur) a été observée dans 15 % des cas (n=4). Les dysmotilités du corps de l’œsophage s’expliquaient par une hypomotilité chez 85 % des patients (n=23), causée par des ondes insignifiantes (74 % [n=20]), des ondes non propagées (11 % [n=3]) ou des ondes de faible amplitude (33 % [n=9]). Des symptômes gastro-œsophagiens ont été constatés chez 66 % des patients obèses (n=35), y compris les brûlures d’estomac (66 % [n=23]), la régurgitation (26 % [n=9]), la dysphagie (43 % [n=15]), les douleurs thoraciques (6 % [n=2]) et la dyspepsie (26 % [n=9]). Chez les patients symptomatiques, 51 % (n=18) présentaient une manométrie normale et 49 % (n=17), une manométrie anormale (statistiquement non significative). Chez les patients asymptomatiques (n=18), 44 % (n=8) avaient une manométrie normale et 56 % (n=10), une manométrie anormale (statistiquement non significative). De plus, il n’y avait pas de différences statistiques entre le groupe ayant une manométrie normale et celui ayant une manométrie anormale en matière de prise de médicaments ou de comorbidités.
CONCLUSION :: La prévalence des dysmotilités œsophagiennes est élevée chez les patients obèses. Les symptômes gastro-intestinaux ne peuvent pas présager de la présence d’une dysmotilité œsophagienne. L’hypomotilité du corps de l’œsophage est la principale dysmotilité, causée notamment par l’absence d’ondes importantes.
Figures
References
-
- World Health Organization (WHO) < www.who.int/topics/obesity/en> (Accessed November 2, 2013).
-
- Nguyen NT, Magno CP, Lane KT, et al. Association of hypertension, diabetes, dyslipidemia, and metabolic syndrome with obesity: Findings from the National Health and Nutrition Examination Survey, 1999 to 2004. J Am Coll Surg. 2008;207:928–34. - PubMed
-
- Jaffin BW, Knoepflmacher P, Greenstein R. High prevalence of asymptomatic motility disorders among morbidly obese patients. Obesity. 1999;9:390–5. - PubMed
-
- Koppman JS, Poggi L, Szomstein S, et al. Esophageal motility disorders in the morbidly obese population. Surg Endosc. 2007;21:761–4. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
