

2012-2013 Seasonal influenza vaccine effectiveness against influenza hospitalizations: results from the global influenza hospital surveillance network
- PMID: 24945510
- PMCID: PMC4063939
- DOI: 10.1371/journal.pone.0100497
2012-2013 Seasonal influenza vaccine effectiveness against influenza hospitalizations: results from the global influenza hospital surveillance network
Erratum in
- PLoS One. 2014;9(9):e107849
Abstract
Background: The effectiveness of currently licensed vaccines against influenza has not been clearly established, especially among individuals at increased risk for complications from influenza. We used a test-negative approach to estimate influenza vaccine effectiveness (IVE) against hospitalization with laboratory-confirmed influenza based on data collected from the Global Influenza Hospital Surveillance Network (GIHSN).
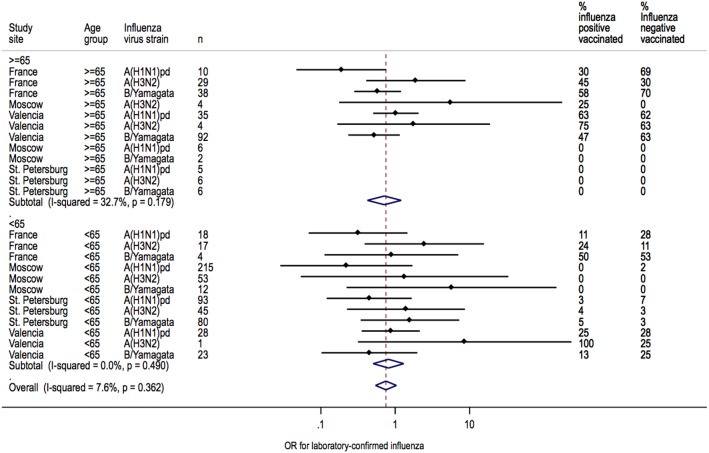
Methods and findings: This was a multi-center, prospective, active surveillance, hospital-based epidemiological study during the 2012-2013 influenza season. Data were collected from hospitals participating in the GIHSN, including five in Spain, five in France, and four in the Russian Federation. Influenza was confirmed by reverse transcription-polymerase chain reaction. IVE against hospitalization for laboratory-confirmed influenza was estimated for adult patients targeted for vaccination and who were swabbed within 7 days of symptom onset. The overall adjusted IVE was 33% (95% confidence interval [CI], 11% to 49%). Point estimates of IVE were 23% (95% CI, -26% to 53%) for influenza A(H1N1)pdm09, 30% (95% CI, -37% to 64%) for influenza A(H3N2), and 43% (95% CI, 17% to 60%) for influenza B/Yamagata. IVE estimates were similar in subjects <65 and ≥65 years of age (35% [95% CI, -15% to 63%] vs.31% [95% CI, 4% to 51%]). Heterogeneity in site-specific IVE estimates was high (I2 = 63.4%) for A(H1N1)pdm09 in patients ≥65 years of age. IVE estimates for influenza B/Yamagata were homogenous (I2 = 0.0%).
Conclusions: These results, which were based on data collected from the GIHSN during the 2012-2013 influenza season, showed that influenza vaccines provided low to moderate protection against hospital admission with laboratory-confirmed influenza in adults targeted for influenza vaccination. In this population, IVE estimates against A(H1N1)pdm09 were sensitive to age group and study site. Influenza vaccination was moderately effective in preventing admissions with influenza B/Yamagata for all sites and age groups.
Conflict of interest statement
Figures





References
-
- Monto AS, Ansaldi F, Aspinall R, McElhaney JE, Montano LF, et al. (2009) Influenza control in the 21st century: Optimizing protection of older adults. Vaccine 27: 5043–5053. - PubMed
-
- Osterholm MT, Kelley NS, Sommer A, Belongia EA (2012) Efficacy and effectiveness of influenza vaccines: a systematic review and meta-analysis. Lancet Infect Dis 12: 36–44. - PubMed
-
- Bragstad K, Emborg H, Fischer TK, Voldstedlund M, Gubbels S, et al... (2013) Low vaccine effectiveness against influenza A(H3N2) virus among elderly people in Denmark in 2012/13–a rapid epidemiological and virological assessment. Euro Surveill 18. - PubMed
-
- McMenamin J, Andrews N, Robertson C, Fleming D, Durnall H, et al... (2013) Effectiveness of seasonal 2012/13 vaccine in preventing laboratory-confirmed influenza infection in primary care in the United Kingdom: mid-season analysis 2012/13. Euro Surveill 18. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
