

Acute hepatitis C in HIV-1 infected Japanese Cohort: single center retrospective cohort study
- PMID: 24945812
- PMCID: PMC4063971
- DOI: 10.1371/journal.pone.0100517
Acute hepatitis C in HIV-1 infected Japanese Cohort: single center retrospective cohort study
Abstract
Objectives: HCV co-infection is a poor prognostic factor in HIV-1-infected patients. Although the number of newly reported patients who show seroconversion is increasing, the clinical features are still unclear, especially in Asian countries.
Design: A single-center retrospective cohort study of patients diagnosed between 2001-2012.
Methods: Acute hepatitis C (AHC) was diagnosed upon detection of high serum ALT (>100 IU) followed by anti-HCV seroconversion. Clinical characteristics, HIV-1-related immunological status and IL-28B genotypes (rs12979860, rs8099917) were collected. We compared these variables between patients with and without spontaneous clearance of HCV and between responders and non-responders to treatment with pegylated interferon (PEG-IFN) plus ribavirin.
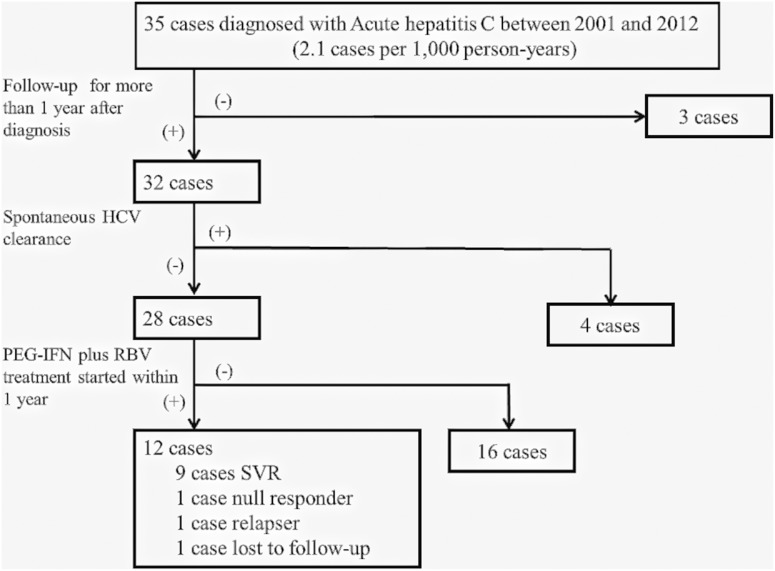
Results: Thirty-five patients were diagnosed with AHC during the study period. The majority (96.9%) were MSM. Three were lost to follow-up. Seventy-five percent of patients with AHC (24/32) were asymptomatic and found incidentally to have high serum ALT. Compared to those who did not show spontaneous clearance, patients with spontaneous HCV viral clearance showed more symptoms and more severe abnormalities related to acute hepatitis. Spontaneous clearance was seen in 4 out of 28 patients with CC+TT genotype, but not in 6 patients with IL-28B CT+TG genotype. PEG-IFN plus ribavirin treatment was initiated in 12 out of 28 cases without spontaneous clearance. The sustained virological response rate was high (81.8%, 9/11), even in cases with CT+TG genotype infected with HCV genotype 1b (SVR 2/2).
Conclusions: Careful attention to AHC is needed in HIV-1-infected MSM. Early diagnosis and PEG-IFN plus ribavirin treatment should be considered for AHC cases.
Conflict of interest statement
Figures
References
-
- Benhamou Y, Bochet M, Di Martino V, Charlotte F, Azria F, et al. (1999) Liver fibrosis progression in human immunodeficiency virus and hepatitis C virus coinfected patients. The Multivirc Group. Hepatology 30: 1054–8. - PubMed
-
- Sauleda S, Juarez A, Esteban JI, Altisent C, Ruiz I, et al. (2001) Interferon and ribavirin combination therapy for chronic hepatitis C in human immunodeficiency virus-infected patients with congenital coagulation disorders. Hepatology 34: 1035–40. - PubMed
-
- Landau A, Batisse D, Piketty C, Duonq Van Huyen JP, Bloch F, et al. (2001) Long-term efficacy of combination therapy with interferon-alpha 2b and ribavirin for severe chronic hepatitis C in HIV-infected patients. AIDS 15: 2149–55. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
