

Hemodynamic directed CPR improves cerebral perfusion pressure and brain tissue oxygenation
- PMID: 24945902
- PMCID: PMC4138228
- DOI: 10.1016/j.resuscitation.2014.05.040
Hemodynamic directed CPR improves cerebral perfusion pressure and brain tissue oxygenation
Abstract
Aim: Advances in cardiopulmonary resuscitation (CPR) have focused on the generation and maintenance of adequate myocardial blood flow to optimize the return of spontaneous circulation and survival. Much of the morbidity associated with cardiac arrest survivors can be attributed to global brain hypoxic ischemic injury. The objective of this study was to compare cerebral physiological variables using a hemodynamic directed resuscitation strategy versus an absolute depth-guided approach in a porcine model of ventricular fibrillation (VF) cardiac arrest.
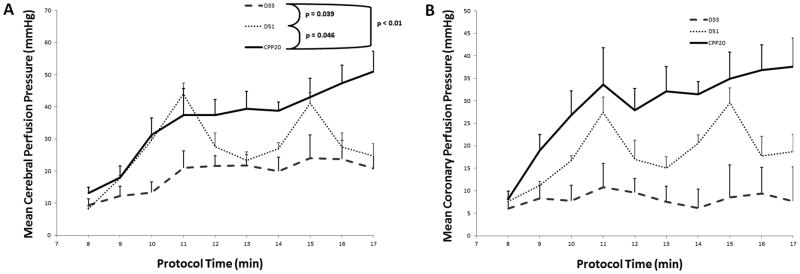
Methods: Intracranial pressure and brain tissue oxygen tension probes were placed in the frontal cortex prior to induction of VF in 21 female 3-month-old swine. After 7 min of VF, animals were randomized to receive one of three resuscitation strategies: (1) hemodynamic directed care (CPP-20): chest compressions (CCs) with depth titrated to a target systolic blood pressure of 100 mmHg and titration of vasopressors to maintain coronary perfusion pressure (CPP)>20 mmHg; (2) depth 33 mm (D33): target CC depth of 33 mm with standard American Heart Association (AHA) epinephrine dosing; or (3) depth 51 mm (D51): target CC depth of 51 mm with standard AHA epinephrine dosing.
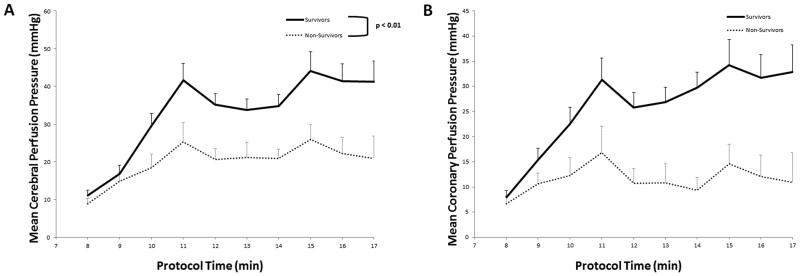
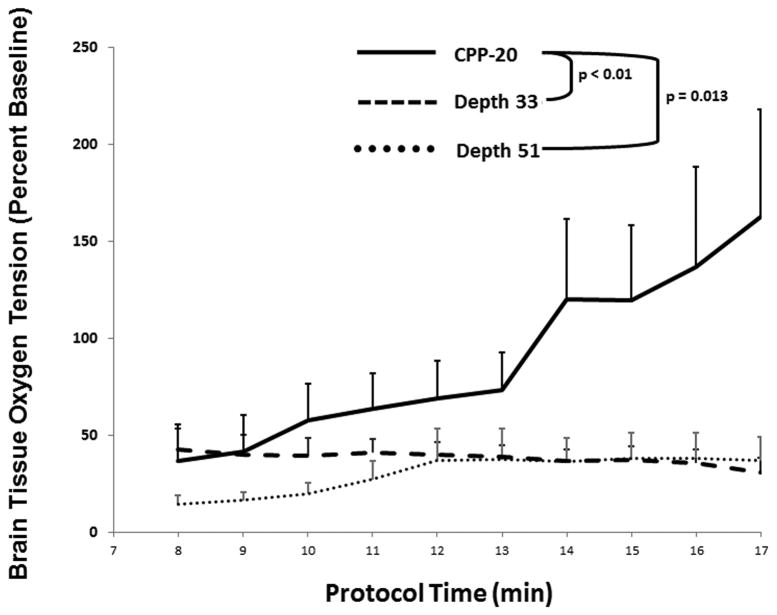
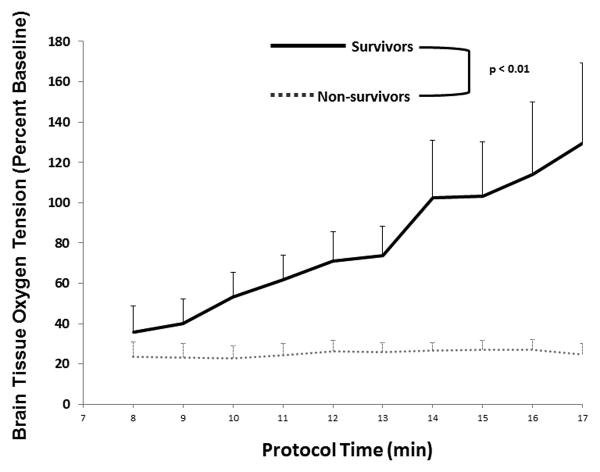
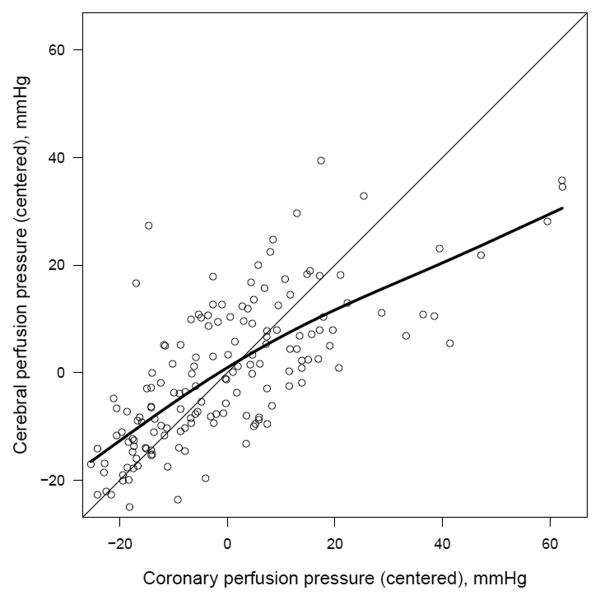
Results: Cerebral perfusion pressures (CerePP) were significantly higher in the CPP-20 group compared to both D33 (p<0.01) and D51 (p=0.046), and higher in survivors compared to non-survivors irrespective of treatment group (p<0.01). Brain tissue oxygen tension was also higher in the CPP-20 group compared to both D33 (p<0.01) and D51 (p=0.013), and higher in survivors compared to non-survivors irrespective of treatment group (p<0.01). Subjects with a CPP>20 mmHg were 2.7 times more likely to have a CerePP>30 mmHg (p<0.001).
Conclusions: Hemodynamic directed resuscitation strategy targeting coronary perfusion pressure>20 mmHg following VF arrest was associated with higher cerebral perfusion pressures and brain tissue oxygen tensions during CPR.
Keywords: Brain tissue oxygen tension; Cardiopulmonary resuscitation; Cerebral perfusion pressure; Coronary perfusion pressure; Intracranial pressure; Ventricular fibrillation.
Copyright © 2014 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Halperin HR, Lee K, Zviman M, Illindala U, Lardo A, Kolandaivelu A, et al. Outcomes from low versus high-flow cardiopulmonary resuscitation in a swine model of cardiac arrest. The American journal of emergency medicine. 2010;28:195–202. - PubMed
-
- Kern KB, Ewy GA, Voorhees WD, Babbs CF, Tacker WA. Myocardial perfusion pressure: a predictor of 24-hour survival during prolonged cardiac arrest in dogs. Resuscitation. 1988;16:241–50. - PubMed
-
- Paradis NA, Martin GB, Rivers EP, Goetting MG, Appleton TJ, Feingold M, et al. Coronary perfusion pressure and the return of spontaneous circulation in human cardiopulmonary resuscitation. JAMA : the journal of the American Medical Association. 1990;263:1106–13. - PubMed
-
- Ralston SH, Voorhees WD, Babbs CF. Intrapulmonary epinephrine during prolonged cardiopulmonary resuscitation: improved regional blood flow and resuscitation in dogs. Annals of emergency medicine. 1984;13:79–86. - PubMed
-
- Berg RA, Sanders AB, Kern KB, Hilwig RW, Heidenreich JW, Porter ME, et al. Adverse hemodynamic effects of interrupting chest compressions for rescue breathing during cardiopulmonary resuscitation for ventricular fibrillation cardiac arrest. Circulation. 2001;104:2465–70. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
