

The fibrotic scar in neurological disorders
- PMID: 24946078
- PMCID: PMC8029481
- DOI: 10.1111/bpa.12162
The fibrotic scar in neurological disorders
Abstract
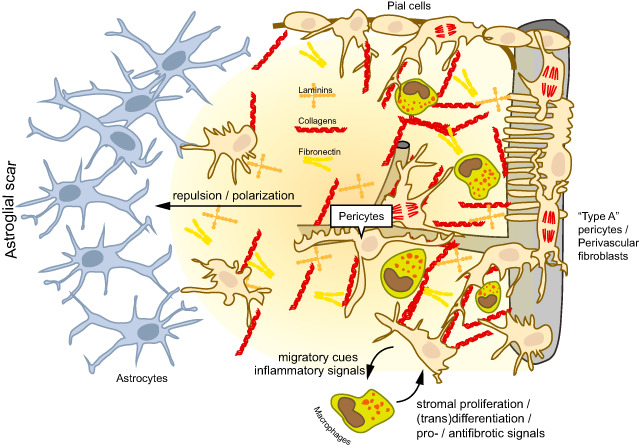
Tissue fibrosis, or scar formation, is a common response to damage in most organs of the body. The central nervous system (CNS) is special in that fibrogenic cells are restricted to vascular and meningeal niches. However, disruption of the blood-brain barrier and inflammation can unleash stromal cells and trigger scar formation. Astroglia segregate from the inflammatory lesion core, and the so-called "glial scar" composed of hypertrophic astrocytes seals off the intact neural tissue from damage. In the lesion core, a second type of "fibrotic scar" develops, which is sensitive to inflammatory mediators. Genetic fate mapping studies suggest that pericytes and perivascular fibroblasts are activated, but other precursor cells may also be involved in generating a transient fibrous extracellular matrix in the CNS. The stromal cells sense inflammation and attract immune cells, which in turn drive myofibroblast transdifferentiation. We believe that the fibrotic scar represents a major barrier to CNS regeneration. Targeting of fibrosis may therefore prove to be a valuable therapeutic strategy for neurological disorders such as stroke, spinal cord injury and multiple sclerosis.
Keywords: (myo)fibroblasts; extracellular matrix; glia; neuroinflammation; pericytes; platelet-derived growth factor receptor.
© 2014 International Society of Neuropathology.
Figures
References
-
- Abnet K, Fawcett JW, Dunnett SB (1991) Interactions between meningeal cells and astrocytes in vivo and in vitro . Brain Res Dev Brain Res 59:187–196. - PubMed
-
- Armulik A, Genové G, Betsholtz C (2011) Pericytes: developmental, physiological, and pathological perspectives, problems, and promises. Dev Cell 21:193–215. - PubMed
-
- Armulik A, Genové G, Mäe M, Nisancioglu MH, Wallgard E, Niaudet C et al (2010) Pericytes regulate the blood‐brain barrier. Nature 468:557–561. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
