

Inhibitory G proteins and their receptors: emerging therapeutic targets for obesity and diabetes
- PMID: 24946790
- PMCID: PMC4081554
- DOI: 10.1038/emm.2014.40
Inhibitory G proteins and their receptors: emerging therapeutic targets for obesity and diabetes
Abstract
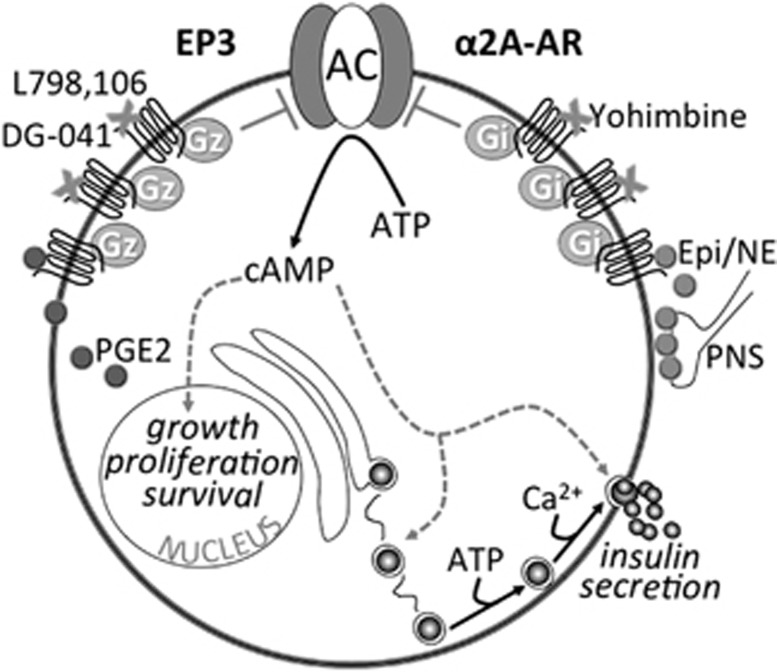
The worldwide prevalence of obesity is steadily increasing, nearly doubling between 1980 and 2008. Obesity is often associated with insulin resistance, a major risk factor for type 2 diabetes mellitus (T2DM): a costly chronic disease and serious public health problem. The underlying cause of T2DM is a failure of the beta cells of the pancreas to continue to produce enough insulin to counteract insulin resistance. Most current T2DM therapeutics do not prevent continued loss of insulin secretion capacity, and those that do have the potential to preserve beta cell mass and function are not effective in all patients. Therefore, developing new methods for preventing and treating obesity and T2DM is very timely and of great significance. There is now considerable literature demonstrating a link between inhibitory guanine nucleotide-binding protein (G protein) and G protein-coupled receptor (GPCR) signaling in insulin-responsive tissues and the pathogenesis of obesity and T2DM. These studies are suggesting new and emerging therapeutic targets for these conditions. In this review, we will discuss inhibitory G proteins and GPCRs that have primary actions in the beta cell and other peripheral sites as therapeutic targets for obesity and T2DM, improving satiety, insulin resistance and/or beta cell biology.
Figures
References
-
- Haffner SM. Epidemiology of type 2 diabetes: risk factors. Diabetes Care. 1998;21 (Suppl 3:C3–C6. - PubMed
-
- DeFronzo RA. Pathogenesis of type 2 (non-insulin dependent) diabetes mellitus: a balanced overview. Diabetologia. 1992;35:389–397. - PubMed
-
- Qatanani M, Lazar MA. Mechanisms of obesity-associated insulin resistance: many choices on the menu. Genes Dev. 2007;21:1443–1455. - PubMed
-
- Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87:4–14. - PubMed
-
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–1053. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical