

Postradiation imaging changes in the CNS: how can we differentiate between treatment effect and disease progression?
- PMID: 24947265
- PMCID: PMC4325371
- DOI: 10.2217/fon.13.271
Postradiation imaging changes in the CNS: how can we differentiate between treatment effect and disease progression?
Abstract
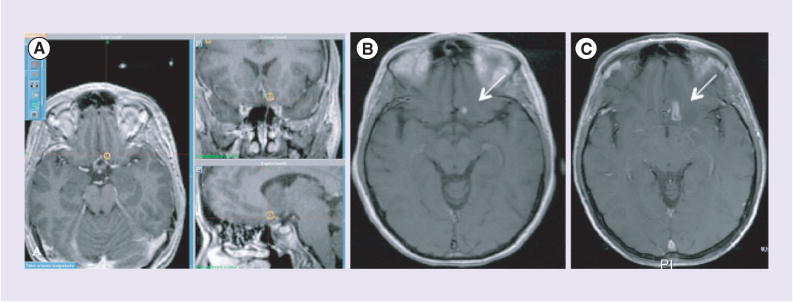
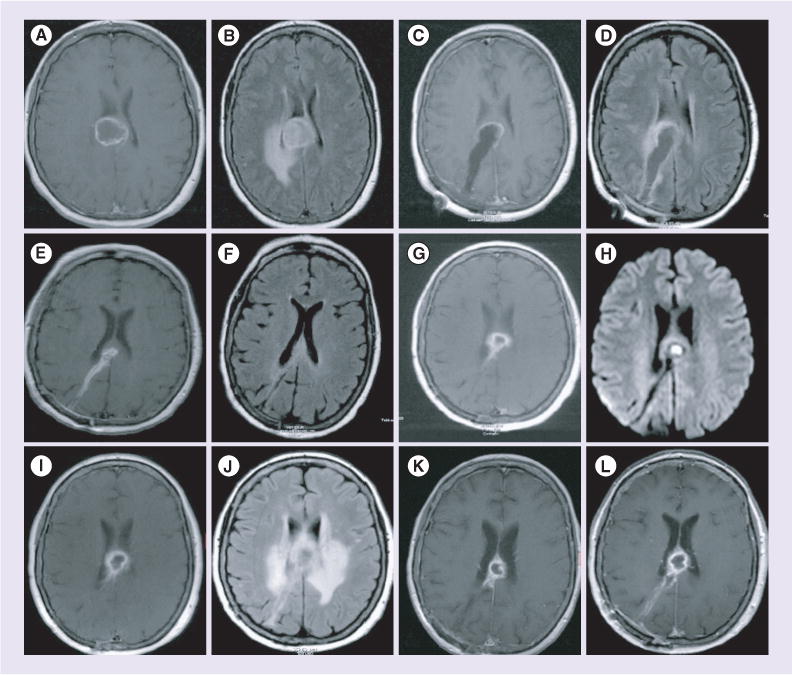
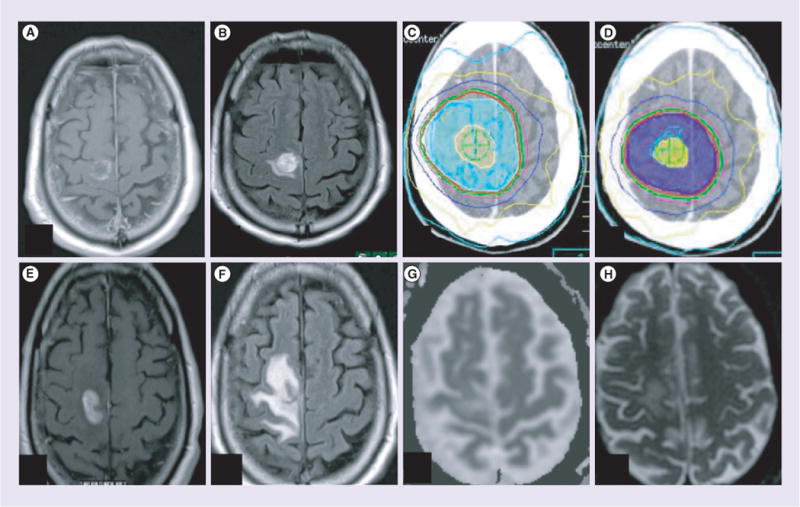
A familiar challenge for neuroradiologists and neuro-oncologists is differentiating between radiation treatment effect and disease progression in the CNS. Both entities are characterized by an increase in contrast enhancement on MRI and present with similar clinical signs and symptoms that may occur either in close temporal proximity to the treatment or later in the disease course. When radiation-related imaging changes or clinical deterioration are mistaken for disease progression, patients may be subject to unnecessary surgery and/or a change from otherwise effective therapy. Similarly, when disease progression is mistaken for treatment effect, a potentially ineffective therapy may be continued in the face of progressive disease. Here we describe the three types of radiation injury to the brain based on the time to development of signs and symptoms--acute, subacute and late--and then review specific imaging changes after intensity-modulated radiation therapy, stereotactic radiosurgery and brachytherapy. We provide an overview of these phenomena in the treatment of a wide range of malignant and benign CNS illnesses. Finally, we review the published data regarding imaging techniques under investigation to address this well-known problem.
Keywords: pseudoprogression; radiation treatment effect; radionecrosis; radiosurgery.
Conflict of interest statement
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Figures
References
-
- Sheline GE. Radiation therapy of brain tumors. Cancer. 1977;39(2 Suppl):873–881. - PubMed
-
- Corn BW, Yousem DM, Scott CB, et al. White matter changes are correlated significantly with radiation dose. Observations from a randomized dose-escalation trial for malignant glioma (Radiation Therapy Oncology Group 83–02) Cancer. 1994;74(10):2828–2835. - PubMed
-
- Emami B, Lyman J, Brown A, et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys. 1991;21(1):109–122. - PubMed
-
- Glass JP, Hwang TL, Leavens ME, Libshitz HI. Cerebral radiation necrosis following treatment of extracranial malignancies. Cancer. 1984;54(9):1966–1972. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical