

Predictors for an unsuccessful INtubation-SURfactant-Extubation procedure: a cohort study
- PMID: 24947477
- PMCID: PMC4072617
- DOI: 10.1186/1471-2431-14-155
Predictors for an unsuccessful INtubation-SURfactant-Extubation procedure: a cohort study
Abstract
Background: The INtubation-SURfactant-Extubation (INSURE) is a procedure that is increasingly being used to treat the respiratory distress syndrome in preterm infants. The objective of this study was to identify predictors for an unsuccessful INSURE procedure.
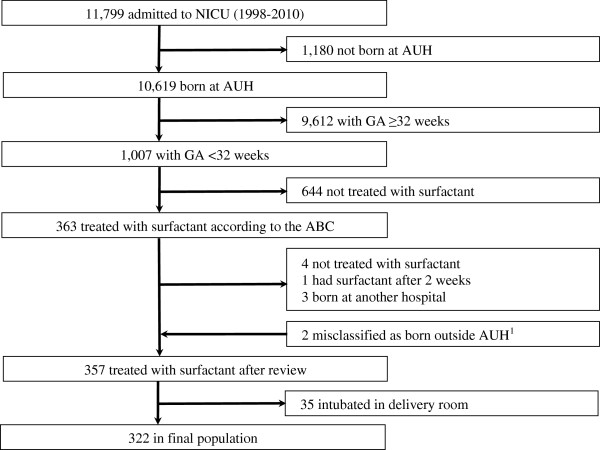
Methods: The neonates included were less than 32 weeks' gestation, treated with surfactant in the neonatal intensive care unit, and born 1998-2010. INSURE was defined as surfactant administration during intubation for less than 2 hours without the need for mechanical ventilation. INSURE success was defined as no re-intubation within 72 hours after INSURE, and INSURE failure was defined as re-intubation within 72 hours after INSURE. An unsuccessful INSURE procedure was either INSURE failure or mechanical ventilation for more than 24 hours immediately after surfactant administration. All predictors were defined a priori and were present before surfactant administration. Multivariate logistic regression was performed.
Results: In total, 322 neonates were included: 31% (n = 100) had INSURE success, 10% (n = 33) had INSURE failure, 49% (n = 158) needed mechanical ventilation for more than 24 hours, and the remaining 10% (n = 31) needed mechanical ventilation for less than 24 hours. Predictors for INSURE failure were low gestational age and hemoglobin below 8.5 mmol/l. Predictors for mechanical ventilation for more than 24 hours were low gestational age, Apgar at 5 minutes below 7, oxygen need above 50%, CO2 pressure above 7 kPa (~53 mmHg), pH below 7.3, lactate above 2.5 mmol/l, need for inotropes, and surfactant administration shortly after birth, whereas preeclampsia reduced the risk.
Conclusions: We identified specific predictors associated with an unsuccessful INSURE procedure. Keeping high-risk neonates with one or several predictors intubated and treated with mechanical ventilation after surfactant may prevent a re-intubation procedure.
Figures
References
-
- Ancora G, Maranella E, Grandi S, Pierantoni L, Guglielmi M, Faldella G. Role of bilevel positive airway pressure in the management of preterm newborns who have received surfactant. Acta Paediatr. 2010;99:1807–1811. - PubMed
-
- Andersen T, Holm HS, Kamper J. Surfactant treatment of newborn infants receiving continuous positive airway pressure treatment. Ugeskr Laeger. 2006;168:3723–3727. - PubMed
-
- Bohlin K, Gudmundsdottir T, Katz-Salamon M, Jonsson B, Blennow M. Implementation of surfactant treatment during continuous positive airway pressure. J Perinatol. 2007;27:422–427. - PubMed
-
- Cherif A, Hachani C, Khrouf N. Risk factors of the failure of surfactant treatment by transient intubation during nasal continuous positive airway pressure in preterm infants. Am J Perinatol. 2008;25:647–652. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
