

Initial independent outcomes from focal impulse and rotor modulation ablation for atrial fibrillation: multicenter FIRM registry
- PMID: 24948520
- PMCID: PMC4282180
- DOI: 10.1111/jce.12474
Initial independent outcomes from focal impulse and rotor modulation ablation for atrial fibrillation: multicenter FIRM registry
Abstract
Introduction: The success of pulmonary vein isolation (PVI) for atrial fibrillation (AF) may be improved if stable AF sources identified by Focal Impulse and Rotor Mapping (FIRM) are also eliminated. The long-term results of this approach are unclear outside the centers where FIRM was developed; thus, we assessed outcomes of FIRM-guided AF ablation in the first cases at 10 experienced centers.
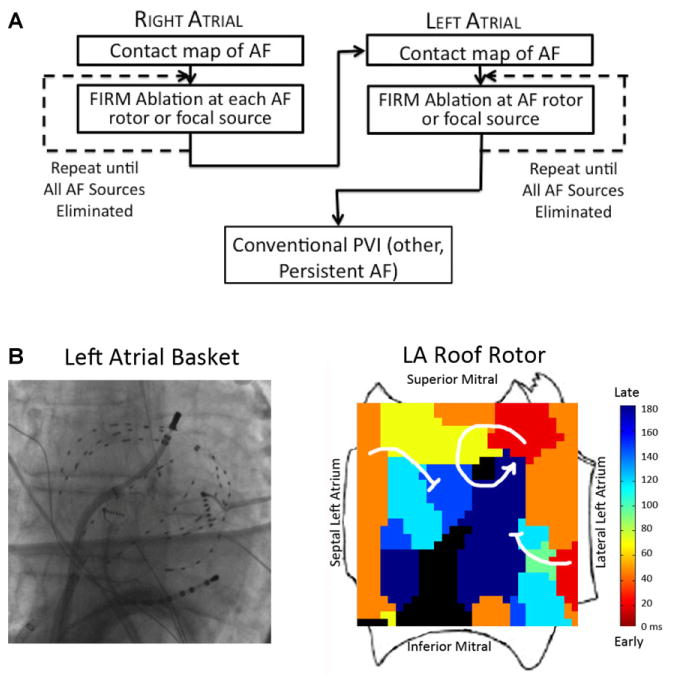
Methods: We prospectively enrolled n = 78 consecutive patients (61 ± 10 years) undergoing FIRM guided ablation for persistent (n = 48), longstanding persistent (n = 7), or paroxysmal (n = 23) AF. AF recordings from both atria with a 64-pole basket catheter were analyzed using a novel mapping system (Rhythm View(TM) ; Topera Inc., CA, USA). Identified rotors/focal sources were ablated, followed by PVI.
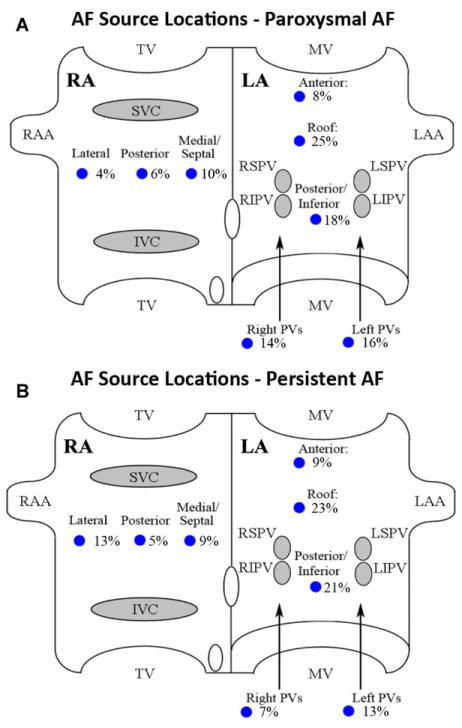
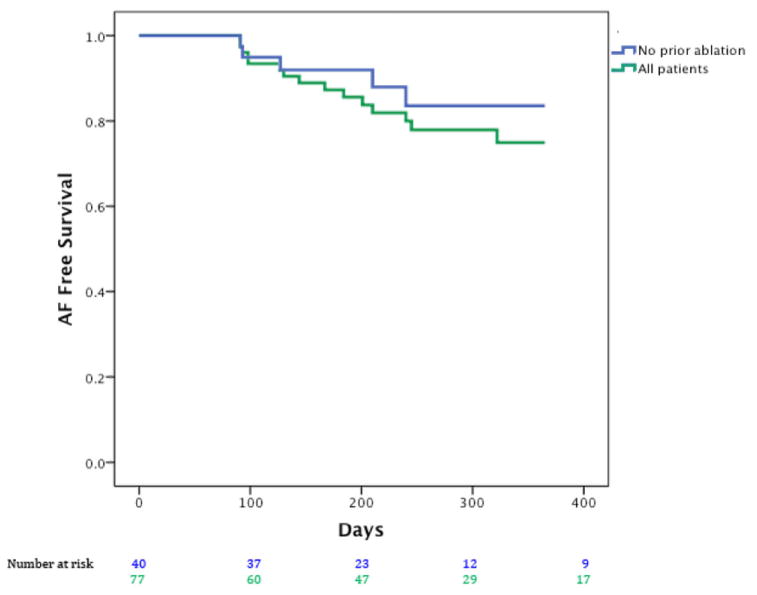
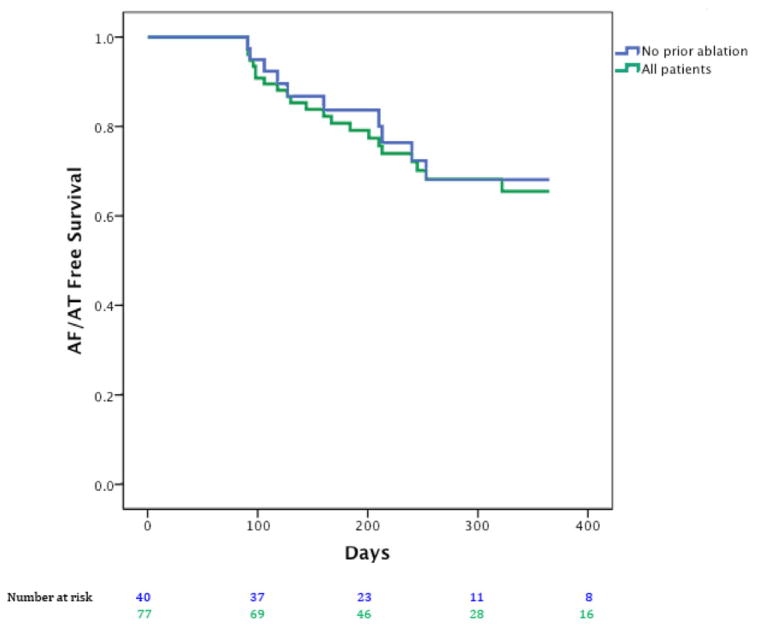
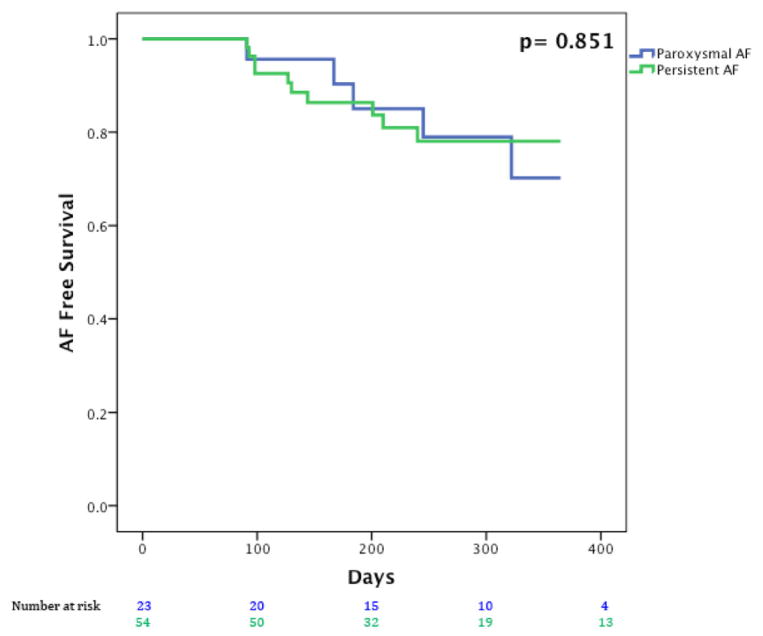
Results: Each institution recruited a median of 6 patients, each of whom showed 2.3 ± 0.9 AF rotors/focal sources in diverse locations. 25.3% of all sources were right atrial (RA), and 50.0% of patients had ≥1 RA source. Ablation of all sources required a total of 16.6 ± 11.7 minutes, followed by PVI. On >1 year follow-up with a 3-month blanking period, 1 patient lost to follow-up (median time to 1st recurrence: 245 days, IQR 145-354), single-procedure freedom from AF was 87.5% (patients without prior ablation; 35/40) and 80.5% (all patients; 62/77) and similar for persistent and paroxysmal AF (P = 0.89).
Conclusions: Elimination of patient-specific AF rotors/focal sources produced freedom-from-AF of ≈80% at 1 year at centers new to FIRM. FIRM-guided ablation has a rapid learning curve, yielding similar results to original FIRM reports in each center's first cases.
Keywords: FIRM-guided ablation; atrial fibrillation; catheter ablation; focal impulse; rotors.
© 2014 Wiley Periodicals, Inc.
Figures
References
-
- Miyasaka Y, Barnes ME, Gersh BJ, Cha SS, Bailey KR, Abhayaratna WP, Seward JB, Tsang TS. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–125. - PubMed
-
- Van Gelder IC, Groenveld HF, Crijns HJ, Tuininga YS, Tijssen JG, Alings AM, Hillege HL, Bergsma-Kadijk JA, Cornel JH, Kamp O, Tukkie R, Bosker HA, Van Veldhuisen DJ, Van den Berg MP. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362:1363–1373. - PubMed
-
- Roy D, Talajic M, Nattel S, Wyse DG, Dorian P, Lee KL, Bourassa MG, Arnold JM, Buxton AE, Camm AJ, Connolly SJ, Dubuc M, Ducharme A, Guerra PG, Hohnloser SH, Lambert J, Le Heuzey JY, O’Hara G, Pedersen OD, Rouleau JL, Singh BN, Stevenson LW, Stevenson WG, Thibault B, Waldo AL. Rhythm control versus rate control for atrial fibrillation and heart failure. N Engl J Med. 2008;358:2667–2677. - PubMed
-
- Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, Kellen JC, Greene HL, Mickel MC, Dalquist JE, Corley SD. A Comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002;347:1825–1833. - PubMed
-
- Nattel S. New ideas about atrial fibrillation 50 years on. Nature. 2002;415:219–226. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
