

Rapid diagnostic tests to improve treatment of malaria and other febrile illnesses: patient randomised effectiveness trial in primary care clinics in Afghanistan
- PMID: 24948695
- PMCID: PMC4064827
- DOI: 10.1136/bmj.g3730
Rapid diagnostic tests to improve treatment of malaria and other febrile illnesses: patient randomised effectiveness trial in primary care clinics in Afghanistan
Abstract
Objective: To assess the impact of rapid diagnostic tests on the diagnostic accuracy and treatment of malaria and non-severe fever in an Asian setting.
Design: Patient randomised trial in primary level clinics.
Setting: Two areas of Afghanistan where Plasmodium vivax and Plasmodium falciparum are endemic; one area with moderate transmission (eastern region) and one with low transmission (northern region).
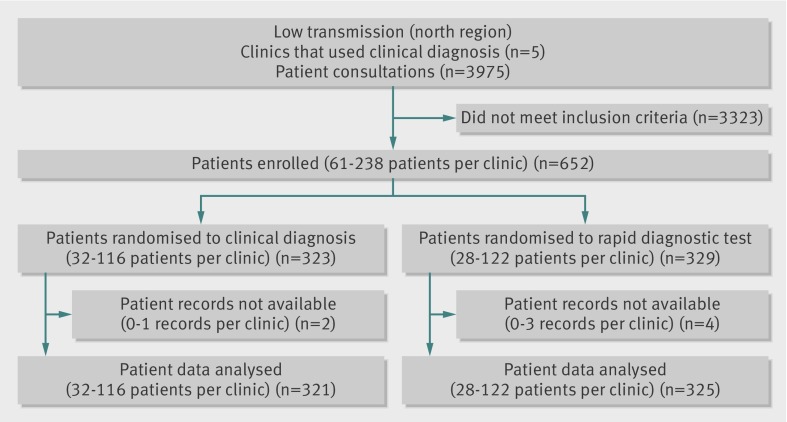
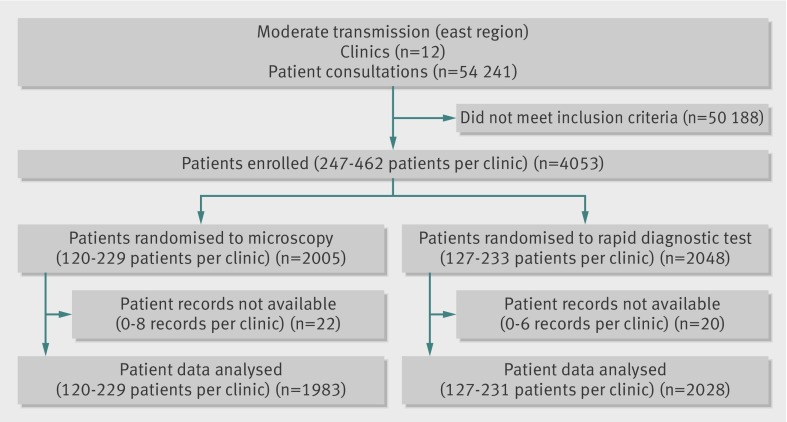
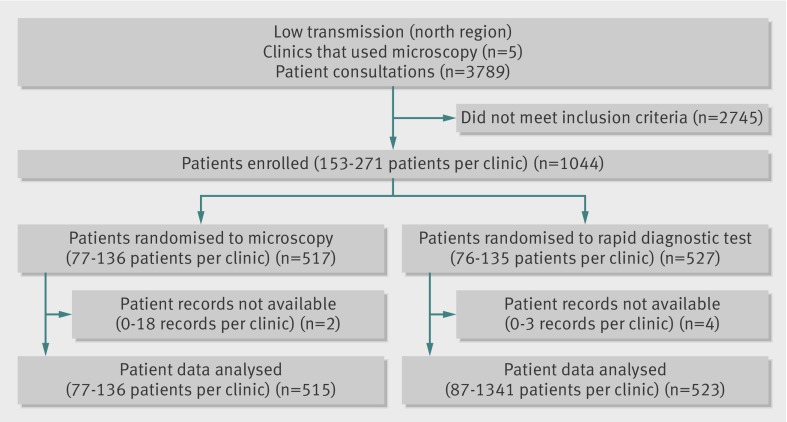
Participants: 5794 patients of all ages with suspected malaria enrolled by 80 clinicians in 22 clinics.
Interventions: Malaria rapid diagnostic tests were compared with clinical diagnosis where no parasite diagnostic test was available, longer established field microscopy, and recently introduced microscopy.
Main outcome measures: Proportion of patients appropriately treated with an antimalarial, defined as patients with P vivax who received chloroquine, patients with P falciparum who received artemisinin based combination therapy, and patients with no malaria parasites who did not receive an antimalarial. Secondary outcomes included diagnostic test accuracy and the proportion of patients negative for malaria who received antibiotics and antimalarials.
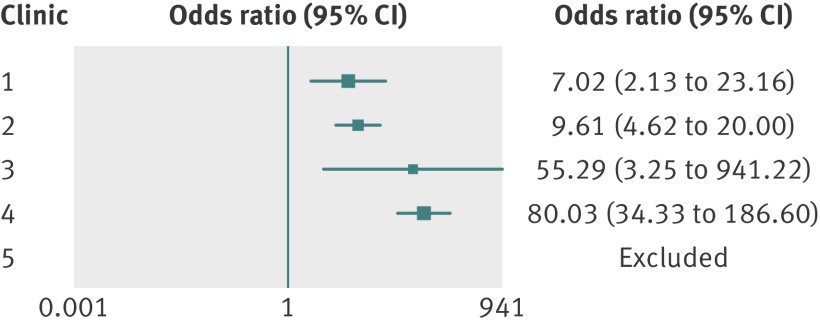
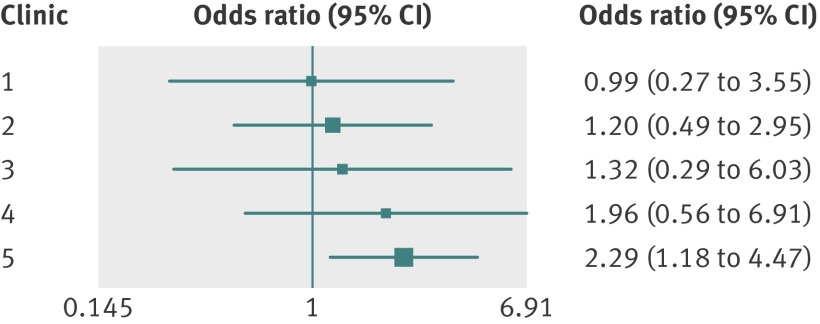
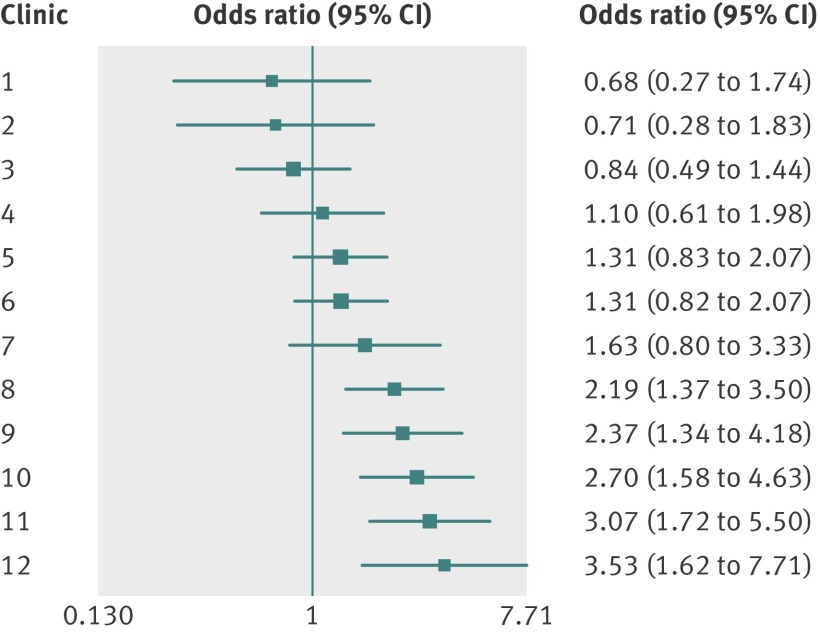
Results: In the low transmission area, comparing rapid diagnostic tests with clinical diagnosis, 65% (212/325) versus 12% (40/321) of febrile patients were appropriately treated for malaria (adjusted odds ratio 92.7, 95% confidence interval 12.4 to 694.1, P<0.001). The proportion of patients who were negative for malaria and received an antibiotic was 57% (185/325) in the rapid diagnostic test arm compared with 14% (46/321) in the clinical diagnosis arm (16.9, 3.8 to 75.4, P<0.001). In the comparison of rapid diagnostic test with microscopy in the moderate transmission area, 83.6% (1696/2028) versus 76.3% (1512/1983) of patients were appropriately treated for malaria (1.70, 1.30 to 2.23, P<0.001). A higher proportion of P falciparum cases received appropriate treatment with artemisinin based combination therapy when malaria was diagnosed by rapid diagnostic test (82%, 58/71 v 32%, 24/76; 9.2, 3.88 to 21.66, P<0.001).
Conclusions: In South and central Asian regions of low to moderate malaria transmission where clinics lack capacity for diagnosis with rapid diagnostic tests or microscopy, the introduction of the tests should be considered to improve clinical care, reduce the overuse of antimalarials, and improve disease surveillance.
Trial registration: ClinicalTrials.gov NCT00935688.
© Leslie et al 2014.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Rapid diagnostic tests for malaria.BMJ. 2014 Jun 19;348:g3846. doi: 10.1136/bmj.g3846. BMJ. 2014. PMID: 24948696 No abstract available.
-
Improving malaria treatment by increasing access to accurate diagnostic tests: test results must guide treatment.Evid Based Med. 2014 Dec;19(6):233. doi: 10.1136/ebmed-2014-110069. Epub 2014 Sep 5. Evid Based Med. 2014. PMID: 25193886 No abstract available.
References
-
- World Health Organization. World malaria report. WHO, 2012.
-
- Joshi R, Colford JM Jr, Reingold AL, Kalantri S. Nonmalarial acute undifferentiated fever in a rural hospital in central India: diagnostic uncertainty and over-treatment with antimalarial agents. Am J Trop Med Hyg 2008;78:393-9. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical