

Overcoming Nonlinear Partial Volume Effects in Known-Component Reconstruction of Cochlear Implants
- PMID: 24949189
- PMCID: PMC4060628
- DOI: 10.1117/12.2007945
Overcoming Nonlinear Partial Volume Effects in Known-Component Reconstruction of Cochlear Implants
Abstract
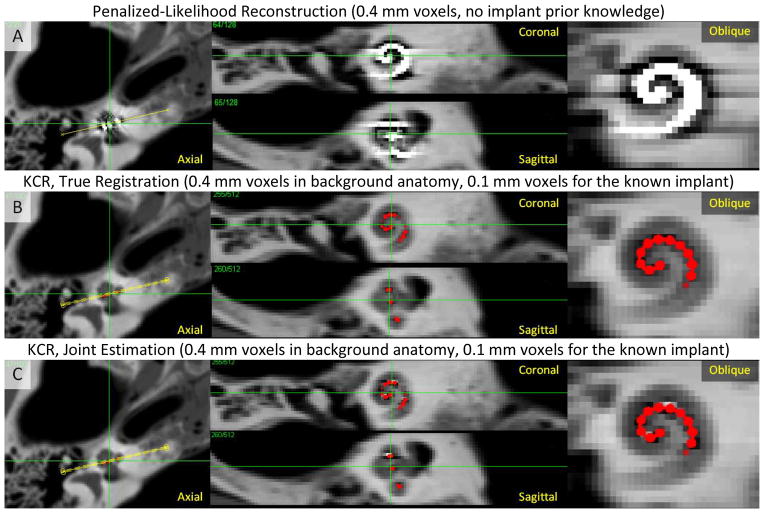
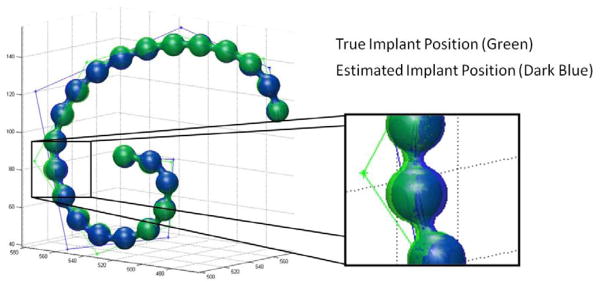
Nonlinear partial volume (NLPV) effects can be significant for objects with large attenuation differences and fine detail structures near the spatial resolution limits of a tomographic system. This is particularly true for small metal devices like cochlear implants. While traditional model-based approaches might alleviate these artifacts through very fine sampling of the image volume and subsampling of rays to each detector element, such solutions can be extremely burdensome in terms of memory and computational requirements. The work presented in this paper leverages the model-based approach called "known-component reconstruction" (KCR) where prior knowledge of a surgical device is integrated into the estimation. In KCR, the parameterization of the object separates the volume into an unknown background anatomy and a known component with unknown registration. Thus, one can model projections of an implant at very high spatial resolution while limiting the spatial resolution of the anatomy - in effect, modeling NLPV effects where they are most significant. We present modifications of the KCR approach that can be used to largely eliminate NLPV artifacts, and demonstrate the efficacy of the modified technique (with improved image quality and accurate implant position estimates) for the cochlear implant imaging scenario.
Figures
References
-
- Noble JH, Dawant BM, Gifford RH, et al. Automatic, Image-based Cochlear Implant Electrode-to-Spiral Ganglion Position Analysis: Implications for Programming. San Diego: 2012.
-
- Bartling SH, Gupta R, Torkos A, et al. Flat-panel volume computed tomography for cochlear implant electrode array examination in isolated temporal bone specimens. Otol Neurotol. 2006;27(4):491–8. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources