

Prediction of difficult laryngoscopy: Extended mallampati score versus the MMT, ULBT and RHTMD
- PMID: 24949304
- PMCID: PMC4063103
- DOI: 10.4103/2277-9175.133270
Prediction of difficult laryngoscopy: Extended mallampati score versus the MMT, ULBT and RHTMD
Abstract
Background: Preoperative using of anatomical landmarks detects potentially difficult laryngoscopies. The main object of the present study was to evaluate the predictive power of Extended Mallampati Score (EMS) in comparison with modified Mallampati test (MMT), the ratio of height to thyromental distance (RHTMD) and the Upper-Lip-Bite test (ULBT) in isolation and combination.
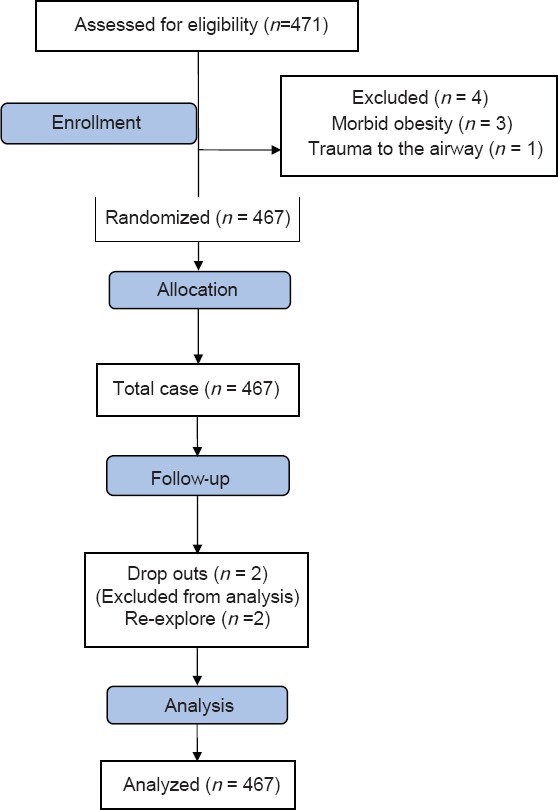
Materials and methods: Four hundred seventy sixadult patients who candidate for elective surgery under general anesthesia requiring endotracheal intubation were included in this study and evaluated based of all four factors before surgery. This study was randomized prospective double - blind. After that, laryngoscopy was performed by an anesthesiologist who didn't involve in preoperative airway assessment and graded based on Cormack and Lehane's classification. We calculated sensitivity, specificity, and area under receiver-operating characteristic (ROC) (AUC) for each score.
Results: The AUCof the ROC was significantly more for the ULBT (AUC = 0.820, P = 0.049) and RHTMD score (AUC = 0.845, P = 0.033) than the EMS (AUC = 0.703). This variable was significantly higher for the EMS compared with MMT (0.703 vs. 0.569, P = 0.046 respectively). There was no significant difference between the AUC of the ROC for the ULBT and the RHTMD score (P = 0.685). The optimalcut-off point for the RHTMD for predicting difficult laryngoscopy was 29.3.
Conclusion: EMS predicted difficult laryngoscopy better than MMT while both ULBT and RHTMD had more power than EMS and MMT in this regard. ULBT and RHTMD had similar predictive value for prediction of difficult laryngoscopy in general population.
Keywords: Difficult laryngoscopy; extended mallampati score; modified mallampati; ratio of patient's height to thyromental distance; upper lip bite test.
Conflict of interest statement
References
-
- Tiret L, Desmonts JM, Hatton F, Vourch G. Complications associated with anaesthesia-a prospective survey in France. Can Anaesth Soc J. 1986;33(3 Pt 1):336–44. - PubMed
-
- Zuercher M, Ummenhofer W. Cardiac arrest during anesthesia. Curr Opin Crit Care. 2008;14:269–74. - PubMed
-
- Braz LG, Módolo NS, do Nascimento P, Jr, Bruschi BA, Castiglia YM, Ganem EM, et al. Perioperative cardiac arrest: A study of 53,718 anaesthetics over 9 yr from a Brazilian teaching hospital. Br J Anaesth. 2006;96:569–75. - PubMed
-
- Arndt M, Benad G. The risks of anesthesia in obstetric interventions. Anaesthesiol Reanim. 1994;19:88–94. - PubMed
-
- Bolander FM. Deaths associated with anaesthesia. Br J Anaesth. 1975;47:36–40. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
