

Transrectal ultrasound - Techniques and outcomes in the management of intestinal endometriosis
- PMID: 24949332
- PMCID: PMC4062201
- DOI: 10.7178/eus.01.005
Transrectal ultrasound - Techniques and outcomes in the management of intestinal endometriosis
Abstract
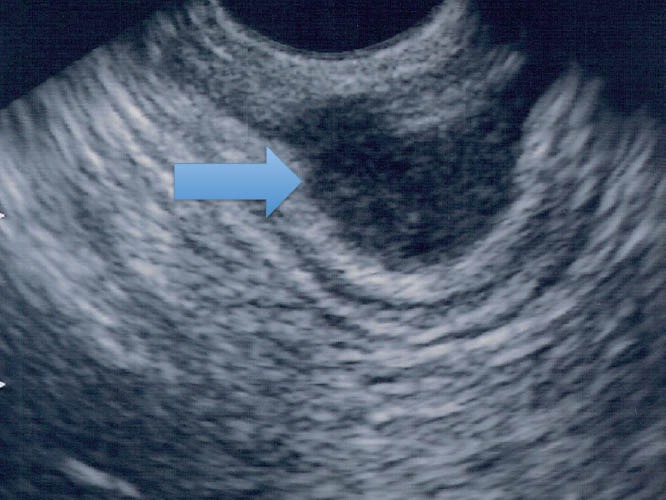
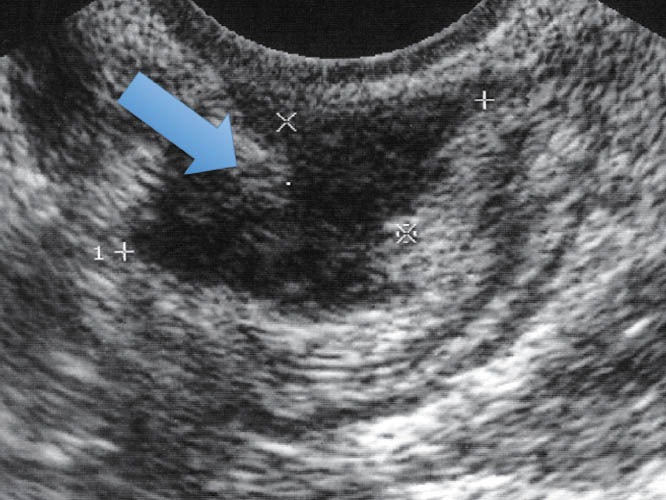
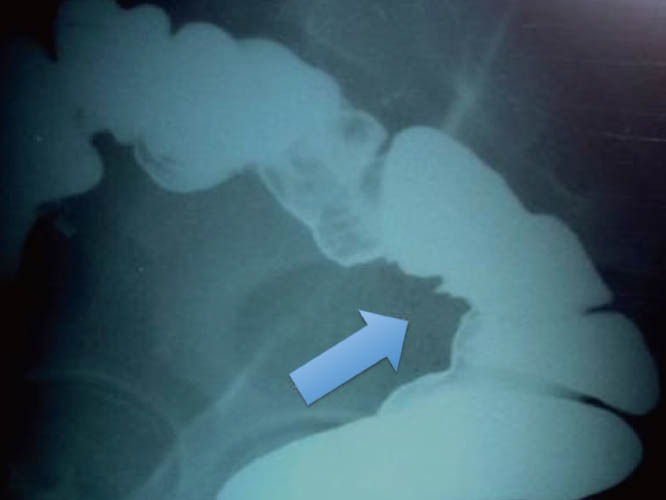
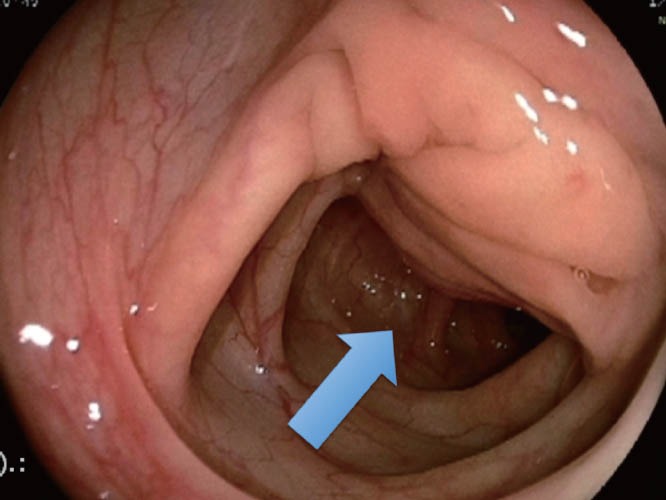
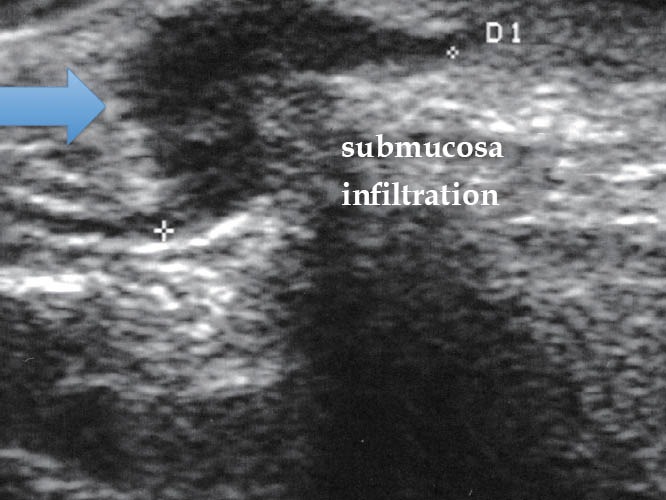
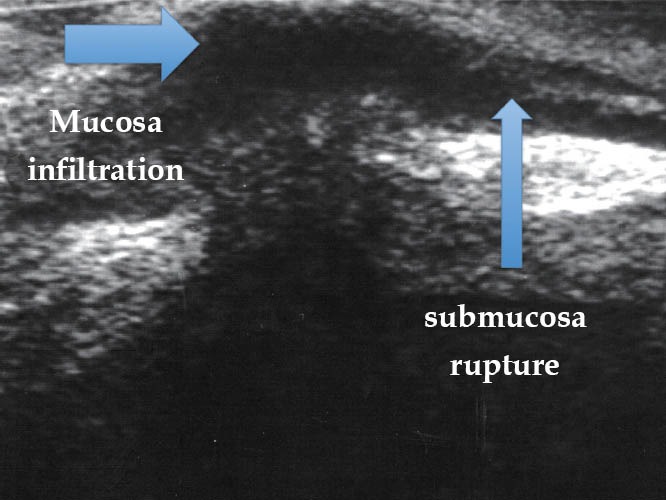
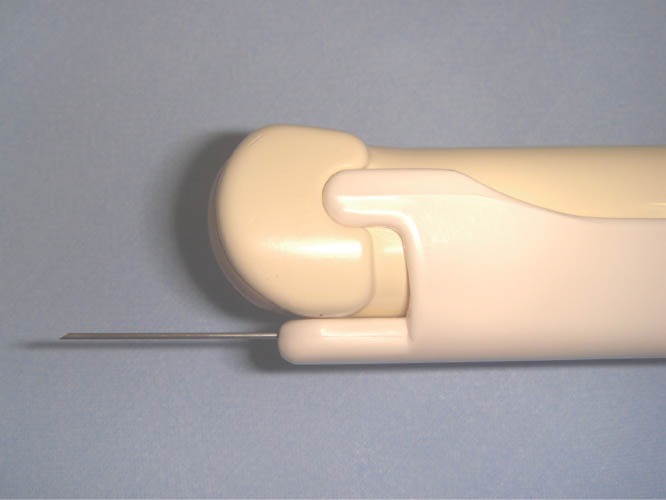
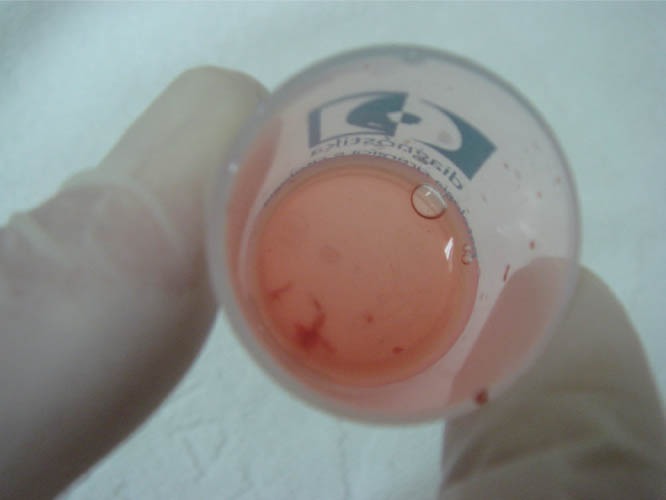
The widespread use of endoscopic ultrasound has facilitated the evaluation of subepithelial and surrounding lesions of the gastrointestinal tract. Deep pelvic endometriosis, with or without infiltration of the intestinal wall, is a frequent disease that can be observed in women in their fertile age. Patients of this disease may present nonspecific signs and symptoms or be completely asymptomatic. Laparoscopic surgical resection of endometriotic lesions is the treatment of choice in symptomatic patients. An accurate preoperative evaluation is indispensable for therapeutic decisions mainly in the suspicion of intestinal wall and/or urinary tract infiltration, and also in cases where we need to establish histological diagnosis or to rule out malignant disease. Diagnostic tools, including transrectal ultrasound, magnetic resonance image, transvaginal ultrasound, barium enema, and colonoscopy, play significant roles in determining the presence, depth, histology, and other relevant data about the extension of the disease. Diagnostic algorithm depends on the clinical presentation, the expertise of the medical team, and the technology available at each institution. This article reviews and discusses relevant clinical points in endometriosis, including techniques and outcomes of the study of the disease through transrectal ultrasound and fine-needle aspiration.
Keywords: endometriosis; endoscopic ultrasonography; fine-needle aspiration.
Figures




Similar articles
-
Comparison of endoscopic ultrasound and magnetic resonance imaging in severe pelvic endometriosis.Gastroenterol Clin Biol. 2000 Dec;24(12):1197-204. Gastroenterol Clin Biol. 2000. PMID: 11173733 English, French.
-
Diagnostic value of endoscopic ultrasonography in pelvic masses with bowel involvement.Therap Adv Gastroenterol. 2023 May 3;16:17562848231163414. doi: 10.1177/17562848231163414. eCollection 2023. Therap Adv Gastroenterol. 2023. PMID: 37153498 Free PMC article. Review.
-
Rectosigmoid endometriosis: endoscopic ultrasound features and clinical implications.Endoscopy. 2000 Jul;32(7):525-30. doi: 10.1055/s-2000-9008. Endoscopy. 2000. PMID: 10917184
-
Rectovaginal endometriosis with nodular smooth muscle metaplasia diagnosed via transrectal ultrasound-guided fine-needle aspiration cytology: An underused minimally invasive diagnostic technique?Diagn Cytopathol. 2023 Oct;51(10):E273-E278. doi: 10.1002/dc.25183. Epub 2023 Jun 15. Diagn Cytopathol. 2023. PMID: 37318678
-
Other imaging techniques: Double-contrast barium enema, endoscopic ultrasonography, multidetector CT enema, and computed tomography colonoscopy.Best Pract Res Clin Obstet Gynaecol. 2021 Mar;71:64-77. doi: 10.1016/j.bpobgyn.2020.05.011. Epub 2020 Jun 8. Best Pract Res Clin Obstet Gynaecol. 2021. PMID: 32698994 Review.
Cited by
-
Rectal cancer staging: Correlation between the evaluation with radial echoendoscope and rigid linear probe.Endosc Ultrasound. 2014 Jul;3(3):161-6. doi: 10.4103/2303-9027.138786. Endosc Ultrasound. 2014. PMID: 25184122 Free PMC article.
-
Rectal endometriosis presenting as toxic megacolon.Autops Case Rep. 2021 Sep 3;11:e2021319. doi: 10.4322/acr.2021.319. eCollection 2021. Autops Case Rep. 2021. PMID: 34540725 Free PMC article.
-
Management of isolated superior mesenteric artery dissection.World J Gastroenterol. 2014 Dec 7;20(45):17179-84. doi: 10.3748/wjg.v20.i45.17179. World J Gastroenterol. 2014. PMID: 25493033 Free PMC article.
-
Nonvisualized palpable bowel endometriotic satellites.Hum Reprod. 2021 Feb 18;36(3):656-665. doi: 10.1093/humrep/deaa340. Hum Reprod. 2021. PMID: 33432338 Free PMC article.
-
Endosonography-assisted diagnosis and therapy of gastrointestinal submucosal tumors.Endosc Ultrasound. 2013 Jul;2(3):125-33. doi: 10.7178/eus.06.003. Endosc Ultrasound. 2013. PMID: 24949380 Free PMC article. Review.
References
-
- Rock JA, Markham SM. Pathogenesis of endometriosis. Lancet. 1992;340:1264–7. - PubMed
-
- Abrão MS, Dias Júnior JA, Podgaec S. Histórico e aspectos epidemiológicos da endometriose: uma doença prevalente e de conhecimento antigo. In: Abrão MS, editor. Endometriose: uma visão contemporânea. Rio de Janeiro: Revinter; 2000. pp. 1–11.
-
- Rochet Y, Lansac J, Drogou F. Les manifestations digestives de l’endométriose. Soc Chir Lyon. 1975;71:247–52.
-
- Sampson JA. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am J Obstet Gynecol. 1927;14:422–69. - PubMed
-
- Jenkinson EL, Brown WH. Endometriosis: a study of 117 cases with special reference to constricting lesions of the rectum and sigmoid colon. JAMA. 1943;122:349–54.
Publication types
LinkOut - more resources
Full Text Sources