

Equity in access to health care services in Italy
- PMID: 24949515
- PMCID: PMC4231580
- DOI: 10.1111/1475-6773.12128
Equity in access to health care services in Italy
Abstract
Objective: To provide new evidence on whether and how patterns of health care utilization deviate from horizontal equity in a country with a universal and egalitarian public health care system: Italy.
Data sources: Secondary analysis of data from the Health Conditions and Health Care Utilization Survey 2005, conducted by the Italian National Institute of Statistics on a probability sample of the noninstitutionalized Italian population.
Study design: Using multilevel logistic regression, we investigated how the probability of utilizing five health care services varies among individuals with equal health status but different SES.
Data collection/extraction: Respondents aged 18 or older at the interview time (n = 103,651).
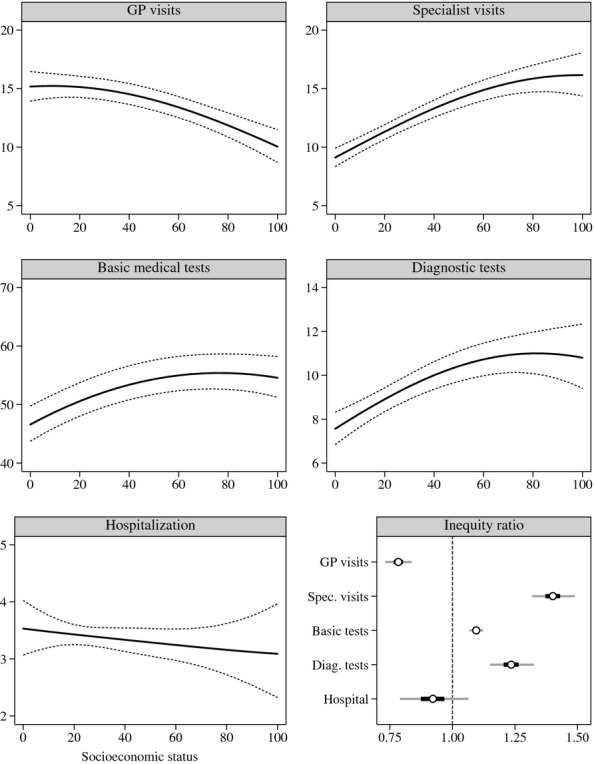
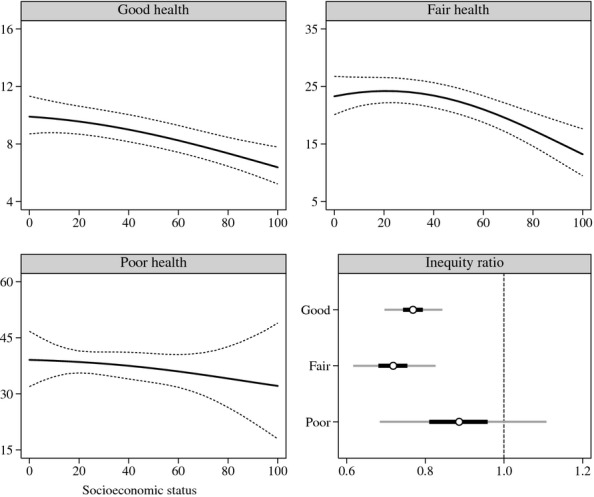
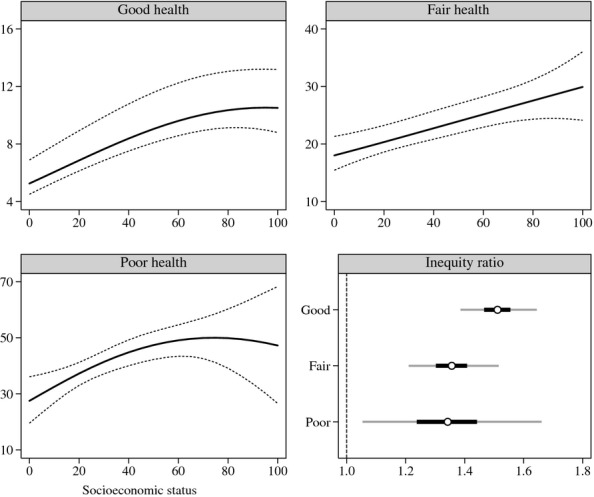
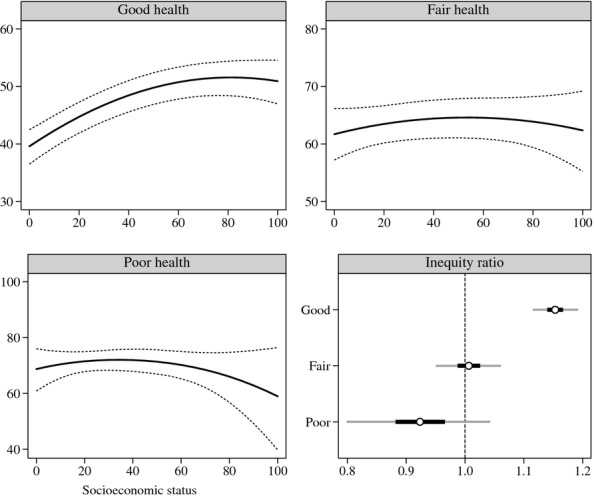
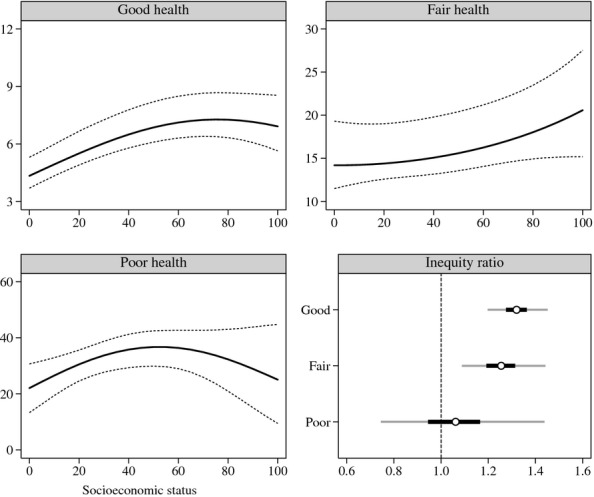
Principal findings: Overall, we found that use of primary care is inequitable in favor of the less well-off, hospitalization is equitable, and use of outpatient specialist care, basic medical tests, and diagnostic services is inequitable in favor of the well-off. Stratifying the analysis by health status, however, we found that the degree of inequity varies according to health status.
Conclusions: Despite its universal and egalitarian public health care system, Italy exhibits a significant degree of SES-related horizontal inequity in health services utilization.
Figures
References
-
- Aday LA, Andersen RM. Development of Indices of Access to Medical Care. Ann Arbor, MI: Health Administration Press; 1975.
-
- Aday LA, Andersen RM. Equity of Access to Medical Care: A Conceptual and Empirical Overview. Medical Care. 1981;19(12 Suppl):4–27. - PubMed
-
- Allin S, Hernández-Quevedo C, Masseria C. Measuring Equity of Access to Health Care. In: Smith PC, Mossialos E, Papanicolas I, Leatherman S, editors. Performance Measurement for Health System Improvement: Experiences, Challenges and Prospects. Cambridge, UK: Cambridge University Press; 2009. pp. 187–221.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
