

Decreased Langerhans cell responses to IL-36γ: altered innate immunity in patients with recurrent respiratory papillomatosis
- PMID: 24950037
- PMCID: PMC4153838
- DOI: 10.2119/molmed.2014.00098
Decreased Langerhans cell responses to IL-36γ: altered innate immunity in patients with recurrent respiratory papillomatosis
Abstract
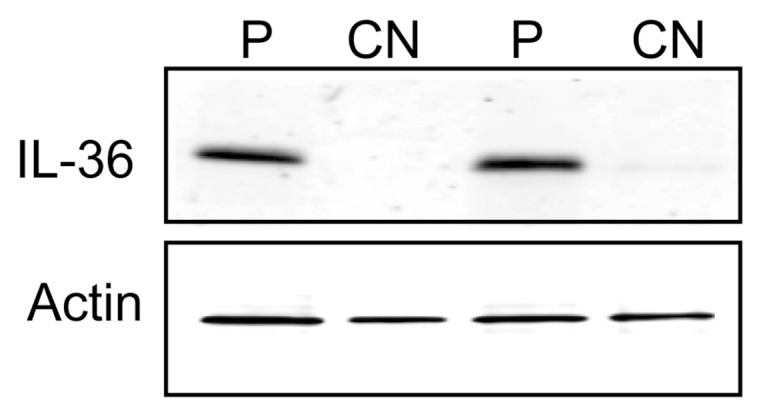
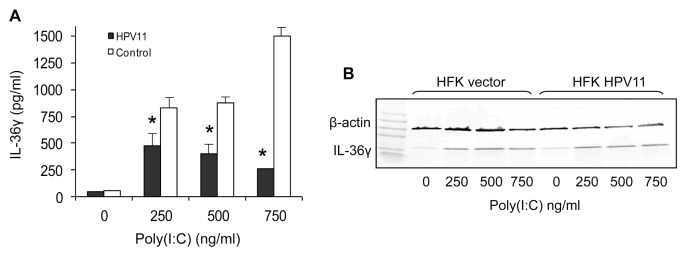
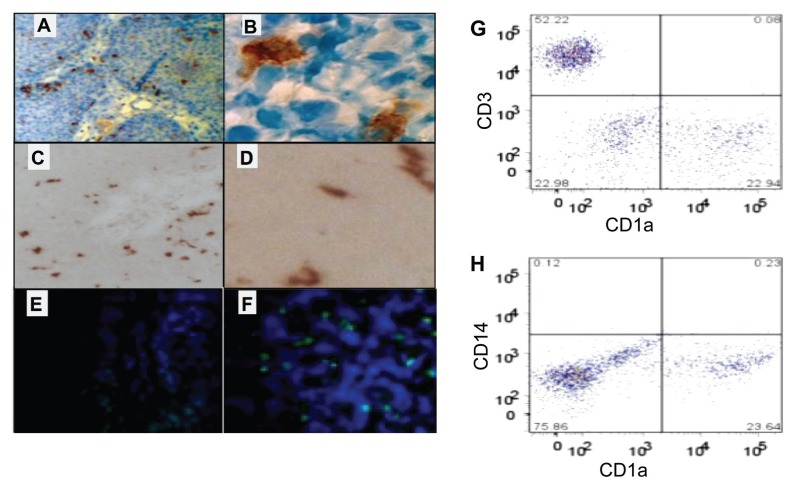
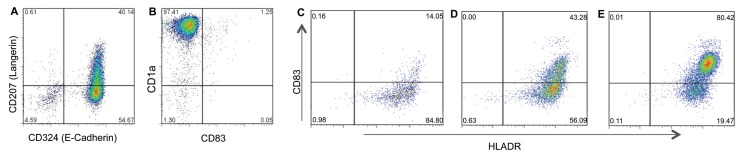
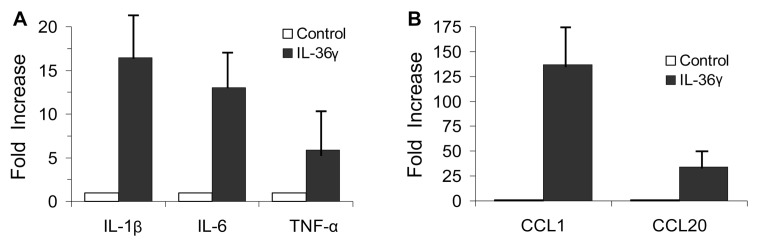
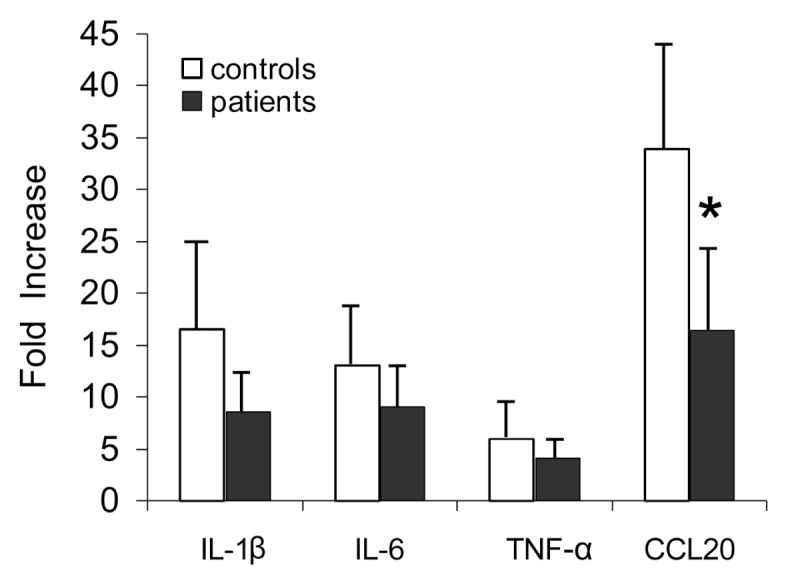
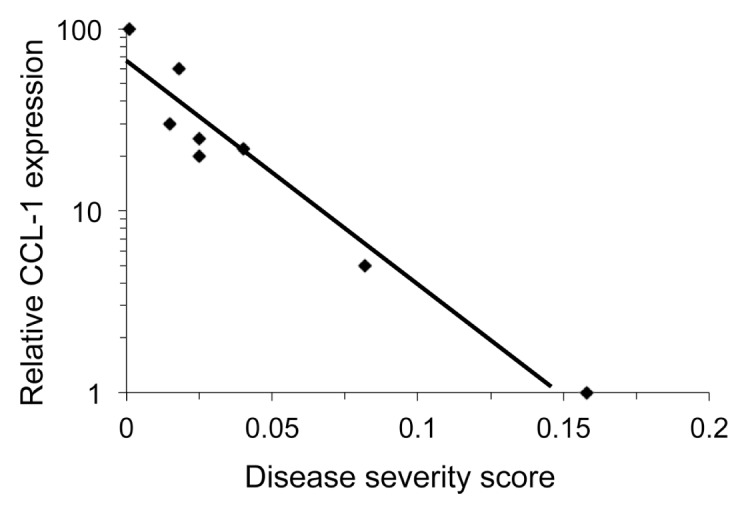
Recurrent respiratory papillomatosis (RRP) is a rare, chronic disease caused by human papillomaviruses (HPVs) types 6 and 11 that is characterized by the polarization of adaptive immune responses that support persistent HPV infection. Respiratory papillomas express elevated mRNA levels of IL-36γ, a proinflammatory cytokine in comparison to autologous clinically normal laryngeal tissues; however there is no evidence of inflammation in these lesions. Consistent with this, respiratory papillomas do not contain TH1-like CD4(+) T-cells or cytotoxic CD8(+) T-cells, but instead contain a predominance of TH2-like and T regulatory cells (Tregs). In addition, papillomas also are infiltrated with immature Langerhans cells (iLCs). In this study, we show that papilloma cells express IL-36γ protein, and that human keratinocytes transduced with HPV11 have reduced IL-36γ secretion. We now provide the first evidence that peripheral blood-derived iLCs respond to IL-36γ by expressing inflammatory cytokines and chemokines. When stimulated with IL-36γ, iLCs from patients with RRP had lower expression levels of the TH2-like chemokine CCL-20 as compared with controls. Patients' iLCs also had decreased steady state levels of CCL-1, which is a proinflammatory chemokine. Moreover, CCL-1 levels in iLCs inversely correlated with the severity of RRP. The combined decrease of TH1- and a TH2-like chemokines by iLCs from patients could have consequences in the priming of IFN-γ expression by CD8(+) T-cells. Taken together, our results suggest that, in RRP, there is a defect in the proinflammatory innate immune responses made by iLCs in response to IL-36γ. The consequence of this defect may lead to persistent HPV infection by failing to support an effective HPV-specific, TH1-like and/or Tc1-like adaptive response, thus resulting in the predominant TH2-like and/or Treg micromilieu present in papillomas.
Figures
Similar articles
-
Altered Monocyte and Langerhans Cell Innate Immunity in Patients With Recurrent Respiratory Papillomatosis (RRP).Front Immunol. 2020 Mar 10;11:336. doi: 10.3389/fimmu.2020.00336. eCollection 2020. Front Immunol. 2020. PMID: 32210959 Free PMC article.
-
Restricted Recruitment of NK Cells with Impaired Function Is Caused by HPV-Driven Immunosuppressive Microenvironment of Papillomas in Aggressive Juvenile-Onset Recurrent Respiratory Papillomatosis Patients.J Virol. 2022 Oct 12;96(19):e0094622. doi: 10.1128/jvi.00946-22. Epub 2022 Sep 26. J Virol. 2022. PMID: 36154611 Free PMC article.
-
Recurrent respiratory papillomatosis: a complex defect in immune responsiveness to human papillomavirus-6 and -11.APMIS. 2010 Jun;118(6-7):455-70. doi: 10.1111/j.1600-0463.2010.02617.x. APMIS. 2010. PMID: 20553528 Free PMC article. Review.
-
Papillomavirus-specific CD4+ T cells exhibit reduced STAT-5 signaling and altered cytokine profiles in patients with recurrent respiratory papillomatosis.J Immunol. 2011 Jun 1;186(11):6633-40. doi: 10.4049/jimmunol.1004181. Epub 2011 Apr 29. J Immunol. 2011. PMID: 21531896 Free PMC article.
-
Immunological tolerance of low-risk HPV in recurrent respiratory papillomatosis.Clin Exp Immunol. 2020 Feb;199(2):131-142. doi: 10.1111/cei.13387. Epub 2019 Oct 31. Clin Exp Immunol. 2020. PMID: 31628850 Free PMC article. Review.
Cited by
-
Pulmonary manifestations of chronic HPV infection in patients with recurrent respiratory papillomatosis.Lancet Respir Med. 2022 Oct;10(10):997-1008. doi: 10.1016/S2213-2600(22)00008-X. Epub 2022 Jul 18. Lancet Respir Med. 2022. PMID: 35863360 Free PMC article. Review.
-
Functional characterization of CD4 and CD8 T cell responses among human papillomavirus infected patients with ano-genital warts.Virusdisease. 2017 Jun;28(2):133-140. doi: 10.1007/s13337-017-0382-8. Epub 2017 Jun 13. Virusdisease. 2017. PMID: 28770238 Free PMC article.
-
How Enhancing Immunity to Low-Risk HPV Could Cure Recurrent Respiratory Papillomatosis.Laryngoscope. 2021 Sep;131(9):2041-2047. doi: 10.1002/lary.29153. Epub 2021 Mar 15. Laryngoscope. 2021. PMID: 33720393 Free PMC article. Review.
-
DNA immunotherapy for recurrent respiratory papillomatosis (RRP): phase 1/2 study assessing efficacy, safety, and immunogenicity of INO-3107.Nat Commun. 2025 Feb 12;16(1):1518. doi: 10.1038/s41467-025-56729-6. Nat Commun. 2025. PMID: 39939590 Free PMC article. Clinical Trial.
-
Homozygous NLRP1 gain-of-function mutation in siblings with a syndromic form of recurrent respiratory papillomatosis.Proc Natl Acad Sci U S A. 2019 Sep 17;116(38):19055-19063. doi: 10.1073/pnas.1906184116. Epub 2019 Sep 4. Proc Natl Acad Sci U S A. 2019. PMID: 31484767 Free PMC article.
References
-
- Bonagura VR, et al. KIR3DS1, KIR2DS1, and KIR2DS5 protect against the development of severe recurrent respiratory papillomatosis (RRP) in HPV-6/11-Infected patients. J. Allergy Clin. Immunol. 2009;123:S165.
-
- Vigne S, et al. IL-36 signaling amplifies Th1 responses by enhancing proliferation and Th1 polarization of naive CD4+ T cells. Blood. 2012;120:3478–87. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
