

Can magnetic resonance imaging findings predict the degree of knee joint laxity in patients undergoing anterior cruciate ligament reconstruction?
- PMID: 24950603
- PMCID: PMC4081463
- DOI: 10.1186/1471-2474-15-214
Can magnetic resonance imaging findings predict the degree of knee joint laxity in patients undergoing anterior cruciate ligament reconstruction?
Abstract
Background: The present study was performed to determine whether MRI findings can predict the degree of knee joint laxity in patients undergoing ACL reconstruction and whether the accuracy of the prediction is affected by the MRI acquisition time.
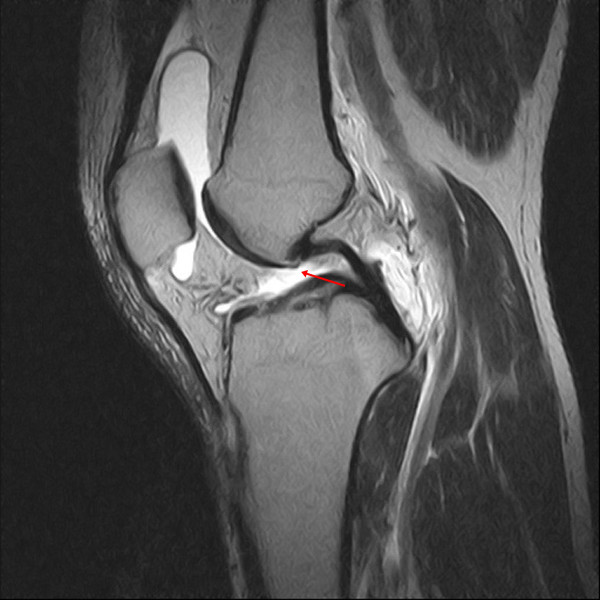
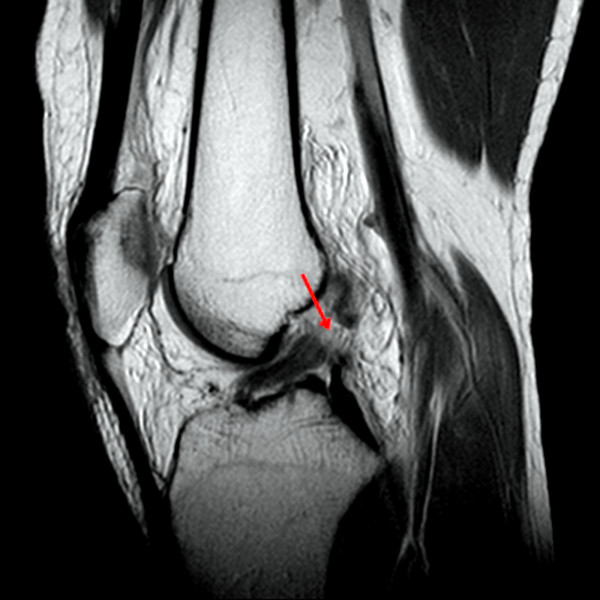
Methods: We assessed prospectively collected data of 154 knees with ACL tears. The presence or absence of four primary findings of ACL tears, i.e., nonvisualization, discontinuity, abnormal signal intensity, and abnormal shape of the ACL, and five secondary findings, i.e., anterior translation of the tibia relative to the femur (≥7 mm), posterior cruciate ligament angle (<105°), bone contusion, Segond fracture, and the deep sulcus sign, were determined. Knee joint laxity was assessed using the Lachman and pivot shift tests. The associations between MRI findings and clinically assessed knee joint laxity were analyzed and compared between subgroups (≤3 months from injury to MRI, 89 knees; >3 months, 65 knees).
Results: Nonvisualization was related to the results of the Lachman test [Odds ratio (OR), 2.6; 95% confidence interval (CI), 1.2-5.5]. Anterior translation of the tibia relative to the femur was related to the results of the pivot shift test (OR, 3.8; 95% CI, 1.6-9.4). In subgroup comparisons of the early and late MRI groups, anterior translation of the tibia relative to the femur was related to the results of the pivot shift test in the early MRI group (OR, 4.5; 95% CI, 1.4-14.4). In contrast, no MRI findings had statistically significant relationships with physical findings in the late MRI group.
Conclusions: Our study indicates that MRI findings may have some usefulness for predicting the grade of knee laxity in patients with symptomatic ACL injury, but its value is limited, especially in patients with a longer time interval between injury and the performance of MRI.
Figures





References
-
- Lerat JL, Moyen BL, Cladiere F, Besse JL, Abidi H. Knee instability after injury to the anterior cruciate ligament. Quantification of the Lachman test. J Bone Joint Surg Br. 2000;82:42–47. - PubMed
-
- Chan WP, Peterfy C, Fritz RC, Genant HK. MR diagnosis of complete tears of the anterior cruciate ligament of the knee: importance of anterior subluxation of the tibia. AJR Am J Roentgenol. 1994;162:355–360. - PubMed
-
- Lee JK, Yao L, Phelps CT, Wirth CR, Czajka J, Lozman J. Anterior cruciate ligament tears: MR imaging compared with arthroscopy and clinical tests. Radiology. 1988;166:861–864. - PubMed
-
- Barenius B, Nordlander M, Ponzer S, Tidermark J, Eriksson K. Quality of life and clinical outcome after anterior cruciate ligament reconstruction using patellar tendon graft or quadrupled semitendinosus graft: an 8-year follow-up of a randomized controlled trial. Am J Sports Med. 2010;38(8):1533–1541. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
