

Azacitidine in 302 patients with WHO-defined acute myeloid leukemia: results from the Austrian Azacitidine Registry of the AGMT-Study Group
- PMID: 24951123
- PMCID: PMC4176957
- DOI: 10.1007/s00277-014-2126-9
Azacitidine in 302 patients with WHO-defined acute myeloid leukemia: results from the Austrian Azacitidine Registry of the AGMT-Study Group
Abstract
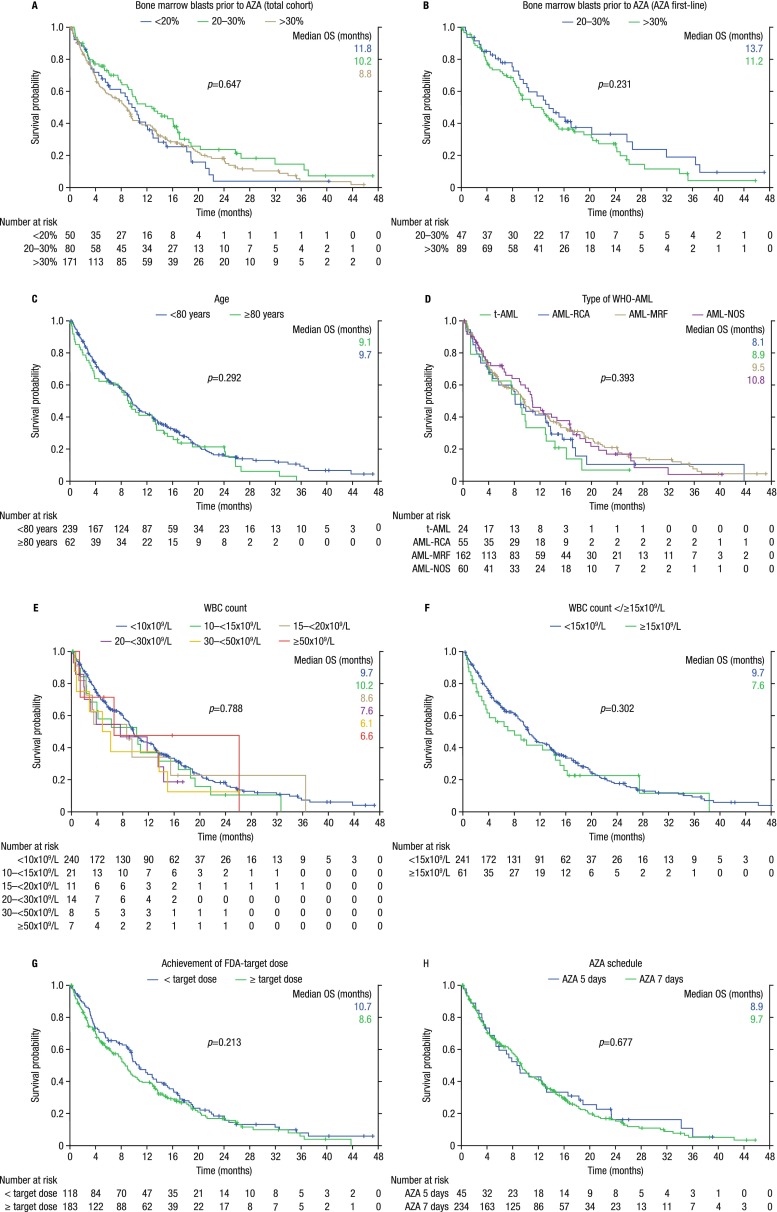
Data on efficacy and safety of azacitidine in acute myeloid leukemia (AML) with >30 % bone marrow (BM) blasts are limited, and the drug can only be used off-label in these patients. We previously reported on the efficacy and safety of azacitidine in 155 AML patients treated within the Austrian Azacitidine Registry (clinicaltrials.gov identifier NCT01595295). We herein update this report with a population almost twice as large (n = 302). This cohort included 172 patients with >30 % BM blasts; 93 % would have been excluded from the pivotal AZA-001 trial (which led to European Medicines Agency (EMA) approval of azacitidine for high-risk myelodysplastic syndromes (MDS) and AML with 20-30 % BM blasts). Despite this much more unfavorable profile, results are encouraging: overall response rate was 48 % in the total cohort and 72 % in patients evaluable according to MDS-IWG-2006 response criteria, respectively. Median OS was 9.6 (95 % CI 8.53-10.7) months. A clinically relevant OS benefit was observed with any form of disease stabilization (marrow stable disease (8.1 months), hematologic improvement (HI) (9.7 months), or the combination thereof (18.9 months)), as compared to patients without response and/or without disease stabilization (3.2 months). Age, white blood cell count, and BM blast count at start of therapy did not influence OS. The baseline factors LDH >225 U/l, ECOG ≥2, comorbidities ≥3, monosomal karyotype, and prior disease-modifying drugs, as well as the response-related factors hematologic improvement and further deepening of response after first response, were significant independent predictors of OS in multivariate analysis. Azacitidine seems effective in WHO-AML, including patients with >30 % BM blasts (currently off-label use). Although currently not regarded as standard form of response assessment in AML, disease stabilization and/or HI should be considered sufficient response to continue treatment with azacitidine.
Figures


References
-
- Fenaux P, Mufti GJ, Hellstrom-Lindberg E, Santini V, Finelli C, Giagounidis A, et al. Efficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: a randomised, open-label, phase III study. Lancet Oncol. 2009;10(3):223–232. doi: 10.1016/S1470-2045(09)70003-8. - DOI - PMC - PubMed
-
- Fenaux P, Mufti GJ, Hellstrom-Lindberg E, Santini V, Gattermann N, Germing U, et al. Azacitidine prolongs overall survival compared with conventional care regimens in elderly patients with low bone marrow blast count acute myeloid leukemia. J Clin Oncol. 2010;28(4):562–569. doi: 10.1200/JCO.2009.23.8329. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
