

Self-awareness in neurodegenerative disease relies on neural structures mediating reward-driven attention
- PMID: 24951639
- PMCID: PMC4107746
- DOI: 10.1093/brain/awu161
Self-awareness in neurodegenerative disease relies on neural structures mediating reward-driven attention
Abstract
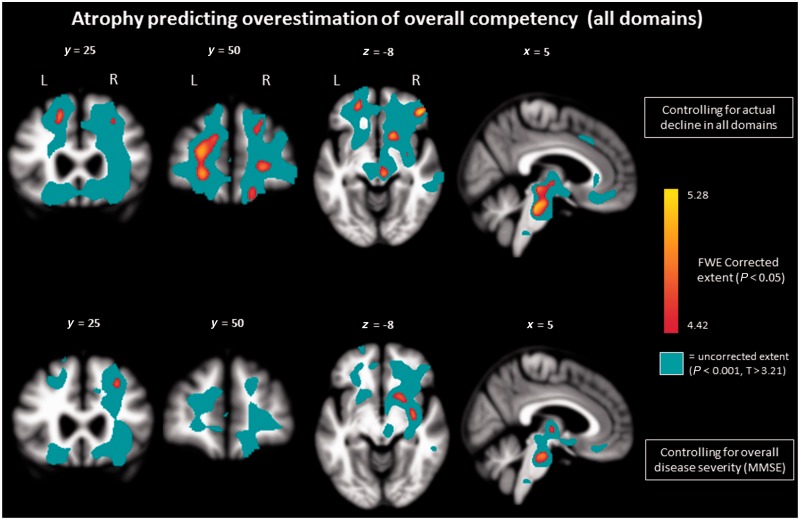
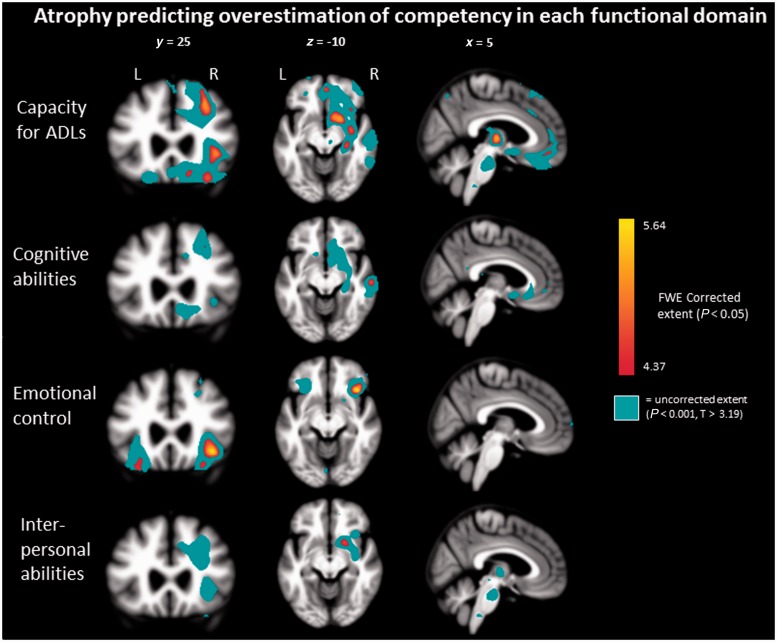
Accurate self-awareness is essential for adapting one's tasks and goals to one's actual abilities. Patients with neurodegenerative diseases, particularly those with right frontal involvement, often present with poor self-awareness of their functional limitations that may exacerbate their already jeopardized decision-making and behaviour. We studied the structural neuroanatomical basis for impaired self-awareness among patients with neurodegenerative disease and healthy older adults. One hundred and twenty-four participants (78 patients with neurodegenerative diseases including Alzheimer's disease, behavioural variant frontotemporal dementia, right-temporal frontotemporal dementia, semantic variant and non-fluent variant primary progressive aphasia, and 46 healthy controls) described themselves on the Patient Competency Rating Scale, rating observable functioning across four domains (daily living activities, cognitive, emotional control, interpersonal). All participants underwent structural magnetic resonance imaging. Informants also described subjects' functioning on the same scale. Self-awareness was measured by comparing self and informant ratings. Group differences in discrepancy scores were analysed using general linear models, controlling for age, sex and disease severity. Compared with controls, patients with behavioural variant frontotemporal dementia overestimated their functioning in all domains, patients with Alzheimer's disease overestimated cognitive and emotional functioning, patients with right-temporal frontotemporal dementia overestimated interpersonal functioning, and patients with non-fluent aphasia overestimated emotional and interpersonal functioning. Patients with semantic variant aphasia did not overestimate functioning on any domain. To examine the neuroanatomic correlates of impaired self-awareness, discrepancy scores were correlated with brain volume using voxel-based morphometry. To identify the unique neural correlates of overlooking versus exaggerating deficits, overestimation and underestimation scores were analysed separately, controlling for age, sex, total intracranial volume and extent of actual functional decline. Atrophy related to overestimating one's functioning included bilateral, right greater than left frontal and subcortical regions, including dorsal superior and middle frontal gyri, lateral and medial orbitofrontal gyri, right anterior insula, putamen, thalamus, and caudate, and midbrain and pons. Thus, our patients' tendency to under-represent their functional decline was related to degeneration of domain-general dorsal frontal regions involved in attention, as well as orbitofrontal and subcortical regions likely involved in assigning a reward value to self-related processing and maintaining accurate self-knowledge. The anatomic correlates of underestimation (right rostral anterior cingulate cortex, uncorrected significance level) were distinct from overestimation and had a substantially smaller effect size. This suggests that underestimation or 'tarnishing' may be influenced by non-structural neurobiological and sociocultural factors, and should not be considered to be on a continuum with overestimation or 'polishing' of functional capacity, which appears to be more directly mediated by neural circuit dysfunction.
Keywords: ageing; attention; awareness; neurodegenerative diseases; voxel based morphometry.
© The Author (2014). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Similar articles
-
Neural substrates of socioemotional self-awareness in neurodegenerative disease.Brain Behav. 2014 Mar;4(2):201-14. doi: 10.1002/brb3.211. Epub 2014 Jan 13. Brain Behav. 2014. PMID: 24683513 Free PMC article.
-
A neural network underlying intentional emotional facial expression in neurodegenerative disease.Neuroimage Clin. 2017 Jan 17;14:672-678. doi: 10.1016/j.nicl.2017.01.016. eCollection 2017. Neuroimage Clin. 2017. PMID: 28373956 Free PMC article.
-
Why do patients with neurodegenerative frontal syndrome fail to answer: 'In what way are an orange and a banana alike?'.Brain. 2015 Feb;138(Pt 2):456-71. doi: 10.1093/brain/awu359. Epub 2014 Dec 16. Brain. 2015. PMID: 25518957 Clinical Trial.
-
Personality and social cognition in neurodegenerative disease.Curr Opin Neurol. 2011 Dec;24(6):550-5. doi: 10.1097/WCO.0b013e32834cd42a. Curr Opin Neurol. 2011. PMID: 22002077 Free PMC article. Review.
-
Neurodegenerative disorders of the human frontal lobes.Handb Clin Neurol. 2019;163:391-410. doi: 10.1016/B978-0-12-804281-6.00021-5. Handb Clin Neurol. 2019. PMID: 31590743 Review.
Cited by
-
Anosognosia in Dementia.Curr Neurol Neurosci Rep. 2016 Sep;16(9):77. doi: 10.1007/s11910-016-0684-z. Curr Neurol Neurosci Rep. 2016. PMID: 27438597 Review.
-
Exploring impaired self-awareness of motor symptoms in Parkinson's disease: Resting-state fMRI correlates and the connection to mindfulness.PLoS One. 2023 Feb 24;18(2):e0279722. doi: 10.1371/journal.pone.0279722. eCollection 2023. PLoS One. 2023. PMID: 36827321 Free PMC article.
-
Fish self-awareness: limits of current knowledge and theoretical expectations.Anim Cogn. 2022 Apr;25(2):447-461. doi: 10.1007/s10071-021-01566-5. Epub 2021 Oct 15. Anim Cogn. 2022. PMID: 34655023 Review.
-
Confabulations in Cases of Dementia: Atypical Early Sign of Alzheimer's Disease or Misleading Feature in Dementia Diagnosis?Front Psychol. 2020 Sep 29;11:553886. doi: 10.3389/fpsyg.2020.553886. eCollection 2020. Front Psychol. 2020. PMID: 33117224 Free PMC article.
-
The right insula contributes to memory awareness in cognitively diverse older adults.Neuropsychologia. 2015 Aug;75:163-9. doi: 10.1016/j.neuropsychologia.2015.05.032. Epub 2015 Jun 3. Neuropsychologia. 2015. PMID: 26049091 Free PMC article.
References
-
- Aalten P, van Valen E, Clare L, Kenny G, Verhey F. Awareness in dementia: a review of clinical correlates. Aging Ment Health. 2005;9:414–22. - PubMed
-
- Adair JC, Gilmore RL, Fennell EB, Gold M, Heilman KM. Anosognosia during intracarotid barbiturate anesthesia: unawareness or amnesia for weakness. Neurology. 1995;45:241–3. - PubMed
-
- Agnew SK, Morris RG. The heterogeneity of anosognosia for memory impairment in Alzheimer's disease: a review of the literature and a proposed model. Aging Ment Health. 1998;2:7–19.
-
- Anton G. Ueber herderkrankungen des gehirnes, welche von patienten selbst nicht wahrgenommen warden. Wiener Klinische Wochenschrift. 1898;11:227–9.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
