

Pulmonary arterial hypertension: the clinical syndrome
- PMID: 24951762
- PMCID: PMC4096686
- DOI: 10.1161/CIRCRESAHA.115.301146
Pulmonary arterial hypertension: the clinical syndrome
Abstract
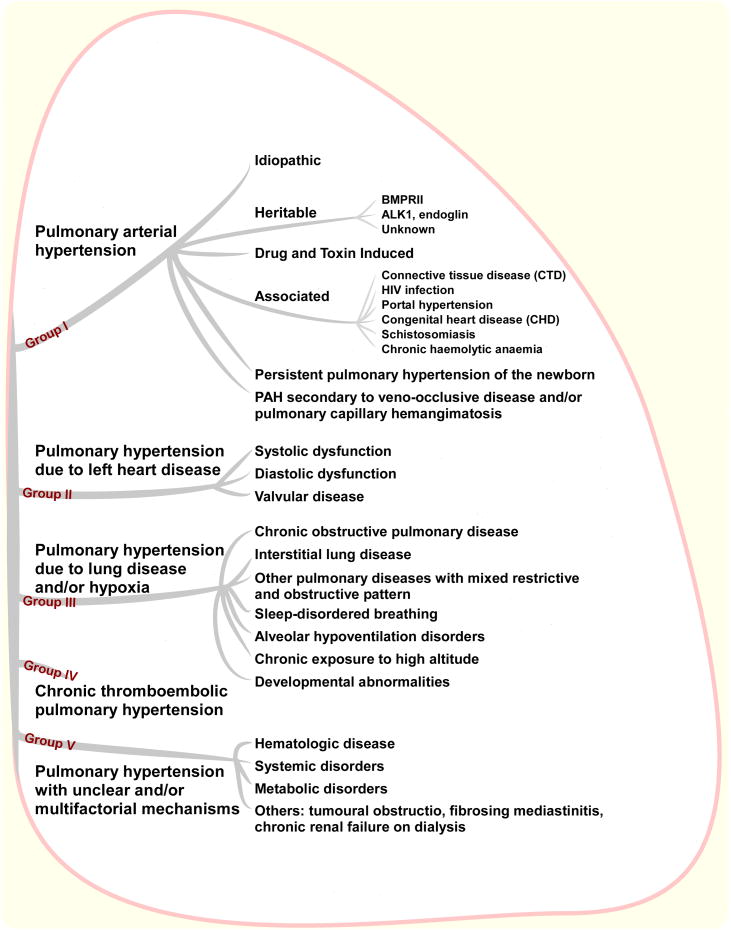
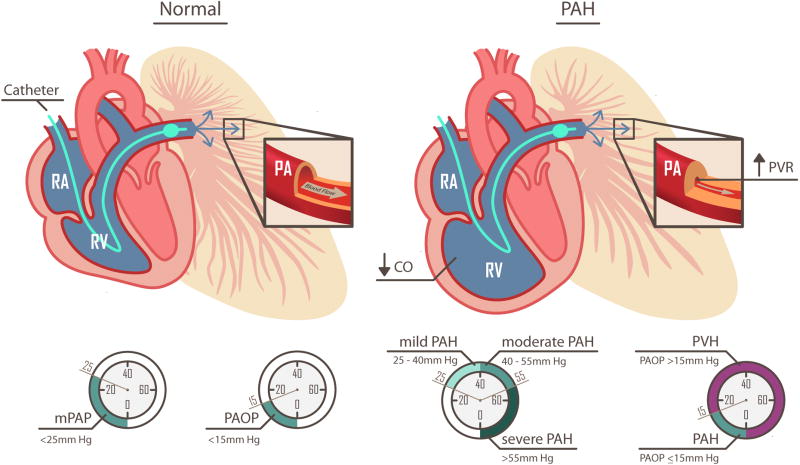
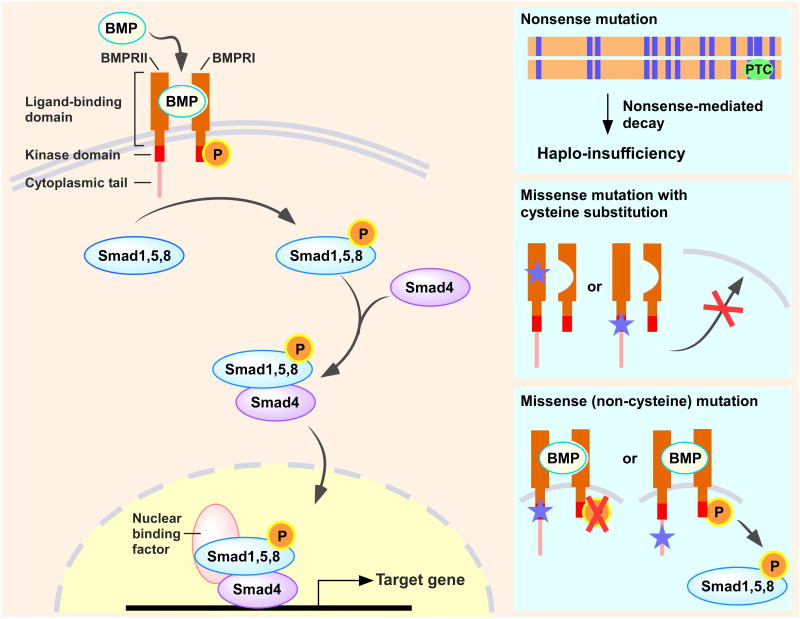
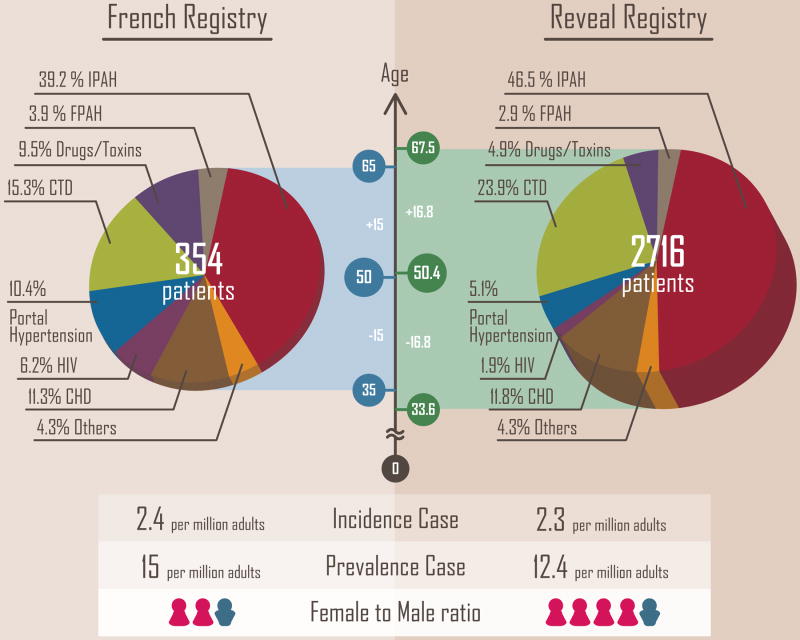
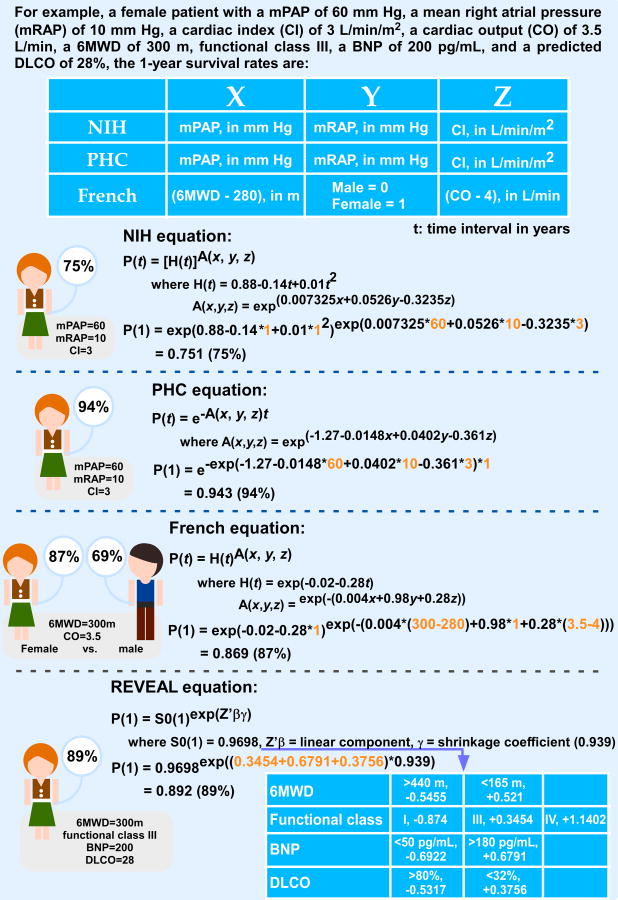
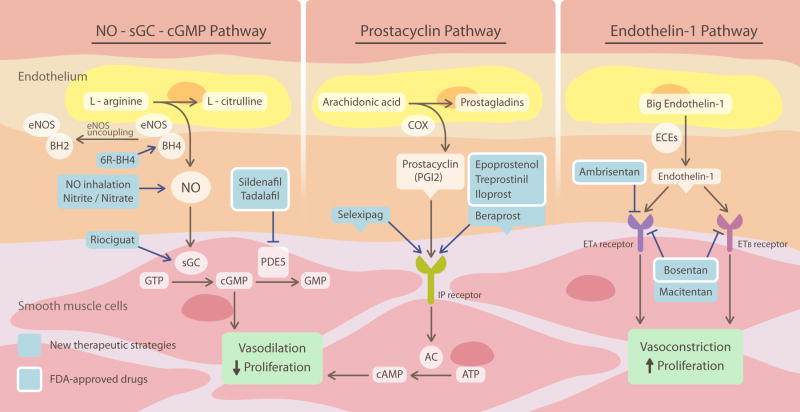
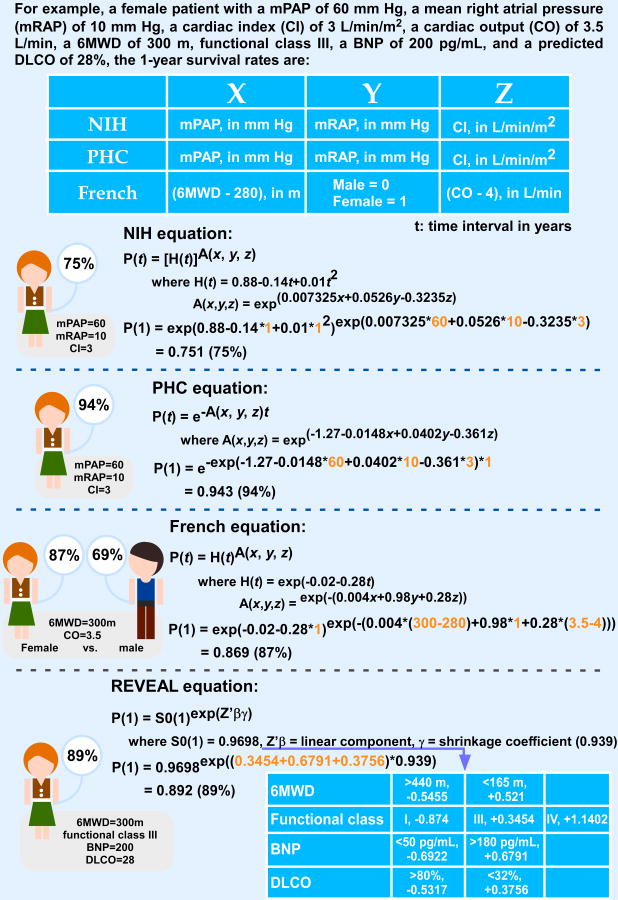
Pulmonary arterial hypertension is a progressive disorder in which endothelial dysfunction and vascular remodeling obstruct small pulmonary arteries, resulting in increased pulmonary vascular resistance and pulmonary pressures. This leads to reduced cardiac output, right heart failure, and ultimately death. In this review, we attempt to answer some important questions commonly asked by patients diagnosed with pulmonary arterial hypertension pertaining to the disease, and aim to provide an explanation in terms of classification, diagnosis, pathophysiology, genetic causes, demographics, and prognostic factors. Furthermore, important molecular pathways that are central to the pathogenesis of pulmonary arterial hypertension are reviewed, including nitric oxide, prostacyclin, endothelin-1, reactive oxygen species, and endothelial and smooth muscle proliferation.
Keywords: hemodynamics; hypertension, pulmonary; nitric oxide.
© 2014 American Heart Association, Inc.
Conflict of interest statement
Figures
References
-
- Archer SL, Djaballah K, Humbert M, Weir KE, Fartoukh M, Dall'ava-Santucci J, Mercier JC, Simonneau G, Dinh-Xuan AT. Nitric oxide deficiency in fenfluramine- and dexfenfluramine-induced pulmonary hypertension. American journal of respiratory and critical care medicine. 1998;158:1061–1067. - PubMed
-
- Rich S, Dantzker DR, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Koerner SK, et al. Primary pulmonary hypertension. A national prospective study. Annals of internal medicine. 1987;107:216–223. - PubMed
-
- Tabuchi A, Mertens M, Kuppe H, Pries AR, Kuebler WM. Intravital microscopy of the murine pulmonary microcirculation. Journal of applied physiology. 2008;104:338–346. - PubMed
-
- Kasner M, Westermann D, Steendijk P, Drose S, Poller W, Schultheiss HP, Tschope C. Left ventricular dysfunction induced by nonsevere idiopathic pulmonary arterial hypertension: A pressure-volume relationship study. American journal of respiratory and critical care medicine. 2012;186:181–189. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
