

The right ventricle in pulmonary arterial hypertension: disorders of metabolism, angiogenesis and adrenergic signaling in right ventricular failure
- PMID: 24951766
- PMCID: PMC4112290
- DOI: 10.1161/CIRCRESAHA.113.301129
The right ventricle in pulmonary arterial hypertension: disorders of metabolism, angiogenesis and adrenergic signaling in right ventricular failure
Abstract
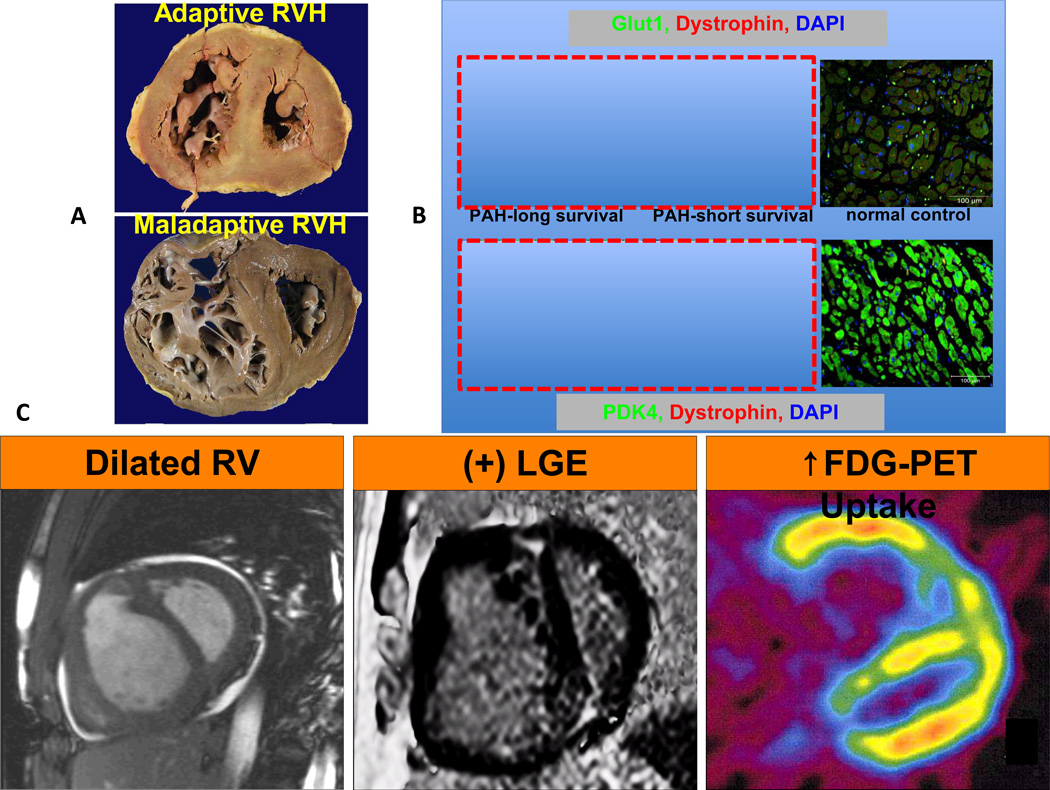
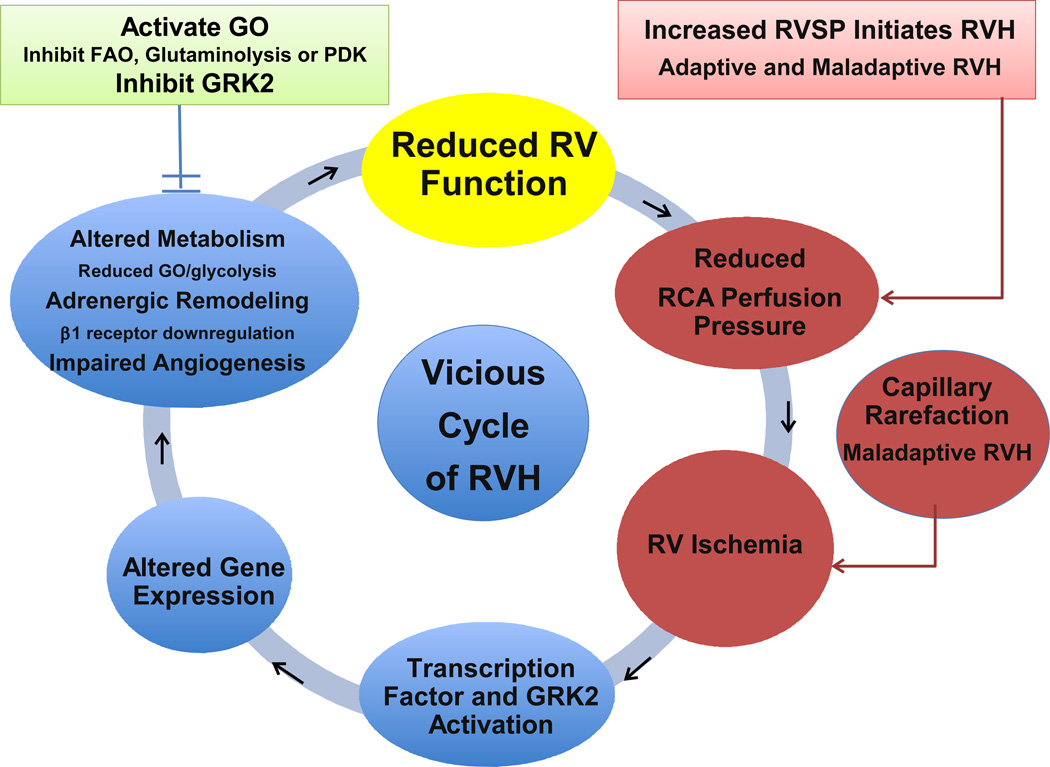
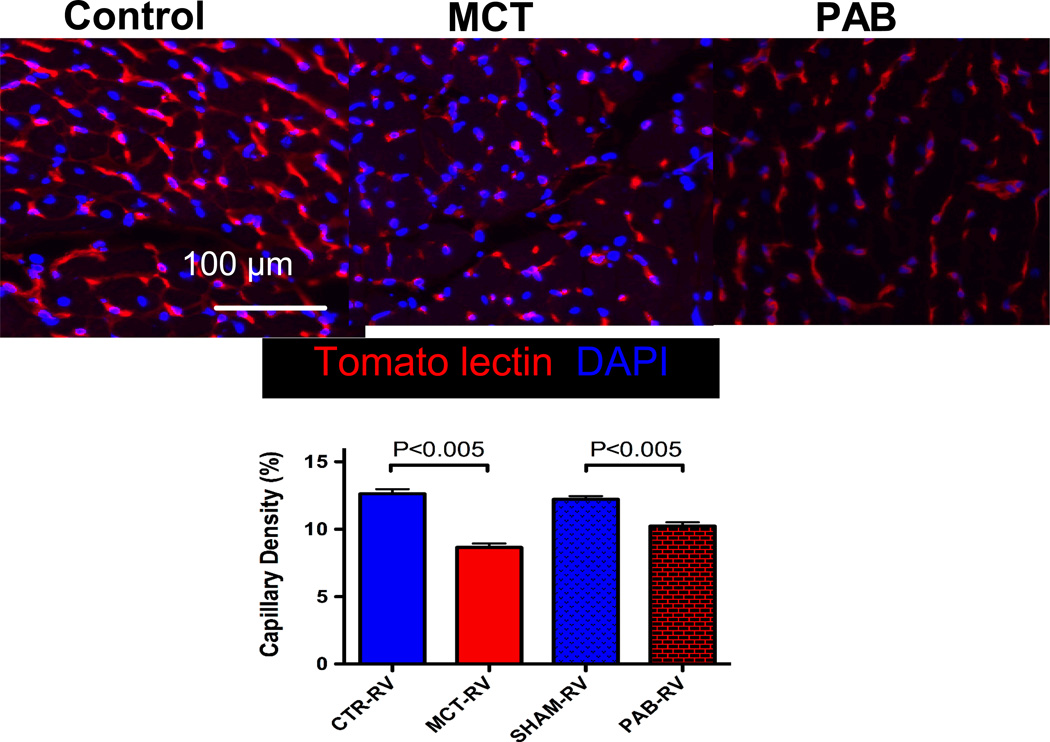
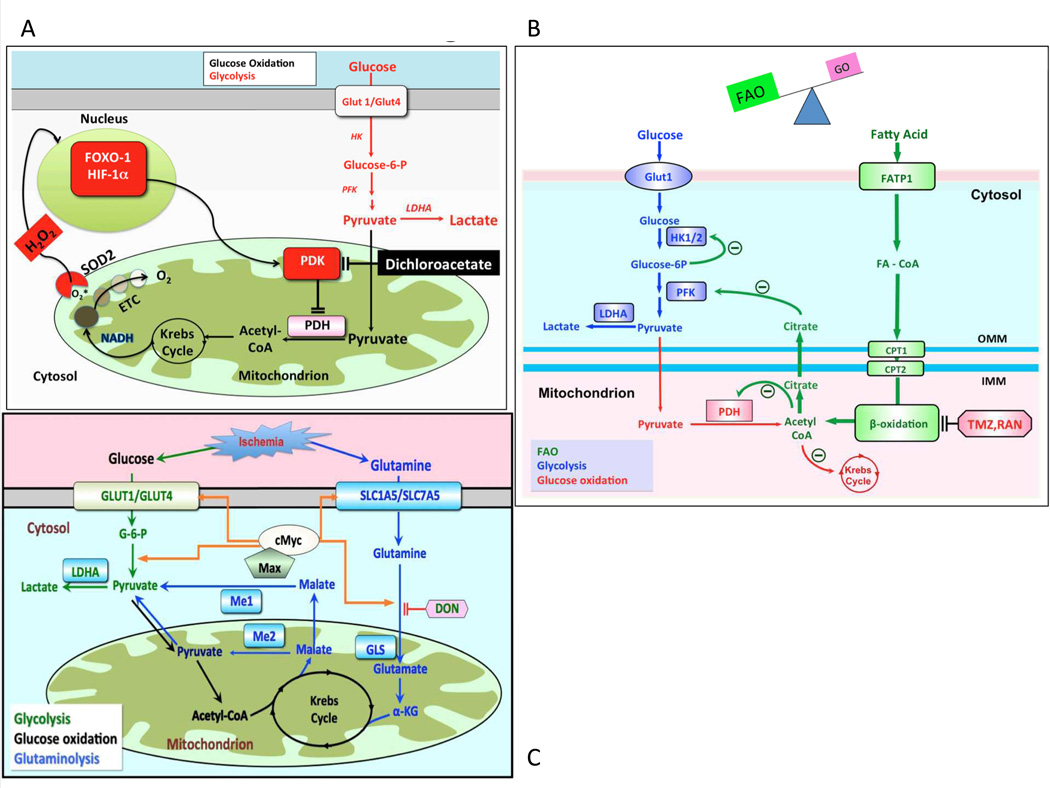
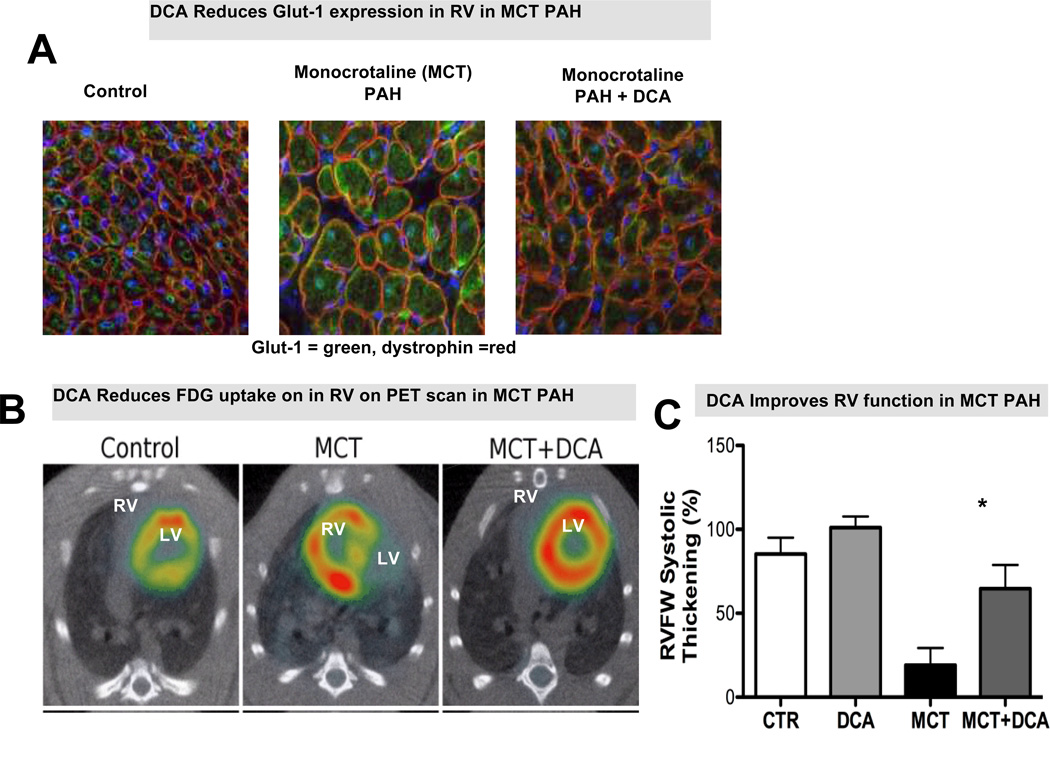
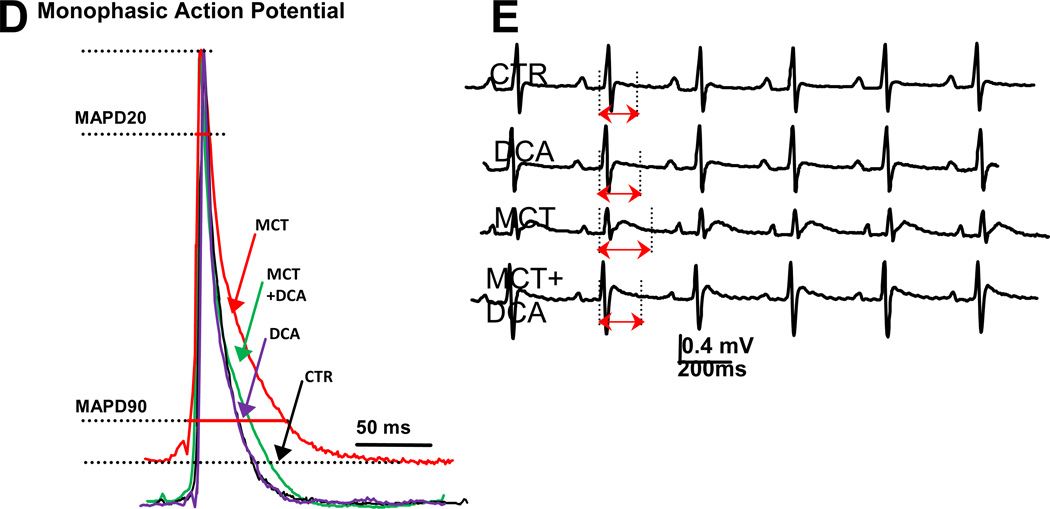
The right ventricle (RV) is the major determinant of functional state and prognosis in pulmonary arterial hypertension. RV hypertrophy (RVH) triggered by pressure overload is initially compensatory but often leads to RV failure. Despite similar RV afterload and mass some patients develop adaptive RVH (concentric with retained RV function), while others develop maladaptive RVH, characterized by dilatation, fibrosis, and RV failure. The differentiation of adaptive versus maladaptive RVH is imprecise, but adaptive RVH is associated with better functional capacity and survival. At the molecular level, maladaptive RVH displays greater impairment of angiogenesis, adrenergic signaling, and metabolism than adaptive RVH, and these derangements often involve the left ventricle. Clinically, maladaptive RVH is characterized by increased N-terminal pro-brain natriuretic peptide levels, troponin release, elevated catecholamine levels, RV dilatation, and late gadolinium enhancement on MRI, increased (18)fluorodeoxyglucose uptake on positron emission tomography, and QTc prolongation on the ECG. In maladaptive RVH there is reduced inotrope responsiveness because of G-protein receptor kinase-mediated downregulation, desensitization, and uncoupling of β-adrenoreceptors. RV ischemia may result from capillary rarefaction or decreased right coronary artery perfusion pressure. Maladaptive RVH shares metabolic abnormalities with cancer including aerobic glycolysis (resulting from a forkhead box protein O1-mediated transcriptional upregulation of pyruvate dehydrogenase kinase), and glutaminolysis (reflecting ischemia-induced cMyc activation). Augmentation of glucose oxidation is beneficial in experimental RVH and can be achieved by inhibition of pyruvate dehydrogenase kinase, fatty acid oxidation, or glutaminolysis. Therapeutic targets in RV failure include chamber-specific abnormalities of metabolism, angiogenesis, adrenergic signaling, and phosphodiesterase-5 expression. The ability to restore RV function in experimental models challenges the dogma that RV failure is irreversible without regression of pulmonary vascular disease.
Keywords: Forkhead box protein O1 (FOXO1); G protein receptor kinase 2 (GRK2); adrenergic receptors; fluorodeoxyglucose; glutamine; glycolysis; pyruvate dehydrogenase complex.
© 2014 American Heart Association, Inc.
Figures
References
-
- Srivastava D, Olson EN. A genetic blueprint for cardiac development. Nature. 2000;407:221–226. - PubMed
-
- Archer SL, Ryan JJ, Rich S, Nathan S, Tsai WK, Patel AR, Fang YH, Piao L. Muscle: Fundamental Biology and Mechanisms of Disease. Academic Press; 2012. The right ventricle: Reemergence of the forgotten ventricle; pp. 537–553.
-
- Dodou E, Verzi MP, Anderson JP, Xu SM, Black BL. Mef2c is a direct transcriptional target of isl1 and gata factors in the anterior heart field during mouse embryonic development. Development. 2004;131:3931–3942. - PubMed
-
- Firpo C, Hoffman JI, Silverman NH. Evaluation of fetal heart dimensions from 12 weeks to term. Am J Cardiol. 2001;87:594–600. - PubMed
-
- Bronicki RA, Baden HP. Pathophysiology of right ventricular failure in pulmonary hypertension. Pediatr Crit Care Med. 2010;11:S15–S22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
