

Adverse prognosis of incidentally detected ambulatory atrial fibrillation. A cohort study
- PMID: 24953051
- PMCID: PMC6374983
- DOI: 10.1160/TH4-04-0383
Adverse prognosis of incidentally detected ambulatory atrial fibrillation. A cohort study
Abstract
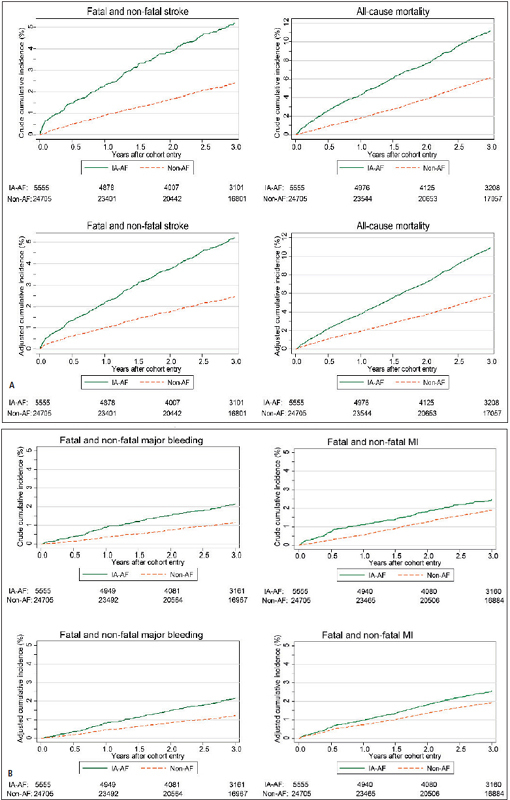
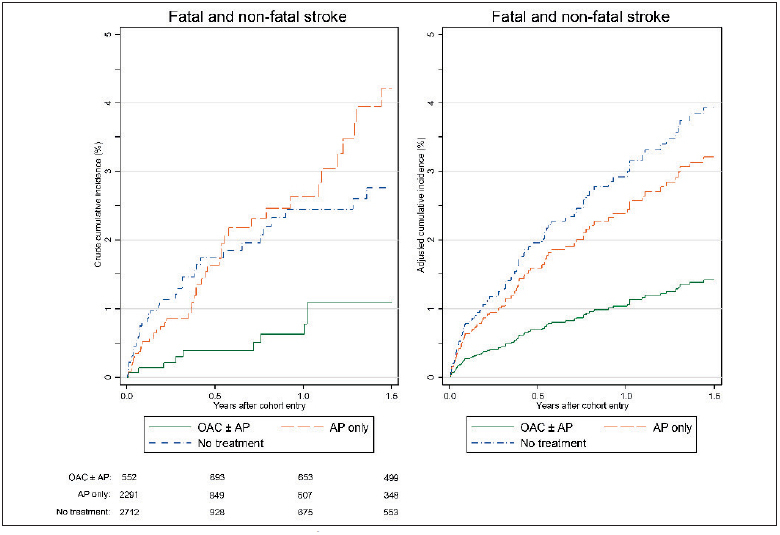
It was the aim of this study to determine prognosis of incidentally detected ambulatory atrial fibrillation (IA-AF) and its response to antithrombotic therapy. We performed a cohort study of 5,555 patients with IA-AF (mean age 70.9 ± 10.1, 38.4% female) and 24,705 age- and gender-matched controls without AF followed three years using UK Clinical Practice Research Datalink. We measured incidence rates of stroke, all-cause mortality, myocardial infarction, major bleeding, and effect of antithrombotic therapy. Patients with IA-AF had mean CHA2DS2VASc score 2.5 ± 1.5, 73% with score ≥2. The stroke incidence rate (IR) was 19.4 (95% confidence interval 17.1 - 21.9)/1,000 person-years vs 8.4 (7.7 - 9.1) in controls (p<0.001), mortality 40.1 (36.8 - 43.6)/1,000 person-years vs 20.9 (19.8 - 22.0) in controls (p<0.001), and myocardial infarction 9.0 (7.5 - 10.8)/1,000 person-years vs 6.5 (5.9 - 7.2) in controls (p<0.001). IRs of all endpoints increased with age. Oral anticoagulant ± antiplatelet therapy received by 51.0% in year following IA-AF was associated with adjusted hazard ratio (HR) of 0.35 (0.17 - 0.71) for stroke, and 0.56 (0.36 - 0.85) for death compared to no therapy, while antiplatelet treatment was associated with a non-significant reduction of HR: 0.81 (0.51 - 1.29) for stroke, and 0.80 (0.55 - 1.15) for death, though both carried a similar small non-significant adjusted excess IR of major bleeding. In conclusion, asymptomatic AF detected incidentally is associated with a significant adverse effect on stroke and death, with reduction in both associated with oral anticoagulant but not antiplatelet treatment. This provides justification to assess cost-effectiveness of community screening to detect unknown AF.
Conflict of interest statement
Figures

References
-
- Miyasaka Y, Barnes ME, Gersh BJ et al.Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–125. - PubMed
-
- Camm AJ, Lip GYH, Caterina RD et al.2012 focused update of the ESC Guidelines for the management of atrial fibrillation. An update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J. 2012;33:2719–2747. - PubMed
-
- Lin HJ, Wolf PA, Kelly-Hayes M et al.Stroke severity in atrial fibrillation. The Framingham Study. Stroke. 1996;27:1760–1764. - PubMed
-
- Benjamin EJMDS, Wolf PAMD, D’Agostino RBP et al.Impact of Atrial Fibrillation on the Risk of Death: The Framingham Heart Study. Circulation. 1998;98:946–952. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical