

Risk factors associated with developing branch retinal vein occlusion among enrollees in a United States managed care plan
- PMID: 24953793
- PMCID: PMC4177949
- DOI: 10.1016/j.ophtha.2014.04.045
Risk factors associated with developing branch retinal vein occlusion among enrollees in a United States managed care plan
Abstract
Purpose: To determine risk factors associated with development of a branch retinal vein occlusion (BRVO) among a large group of managed-care plan beneficiaries in the United States.
Design: Retrospective, longitudinal cohort study.
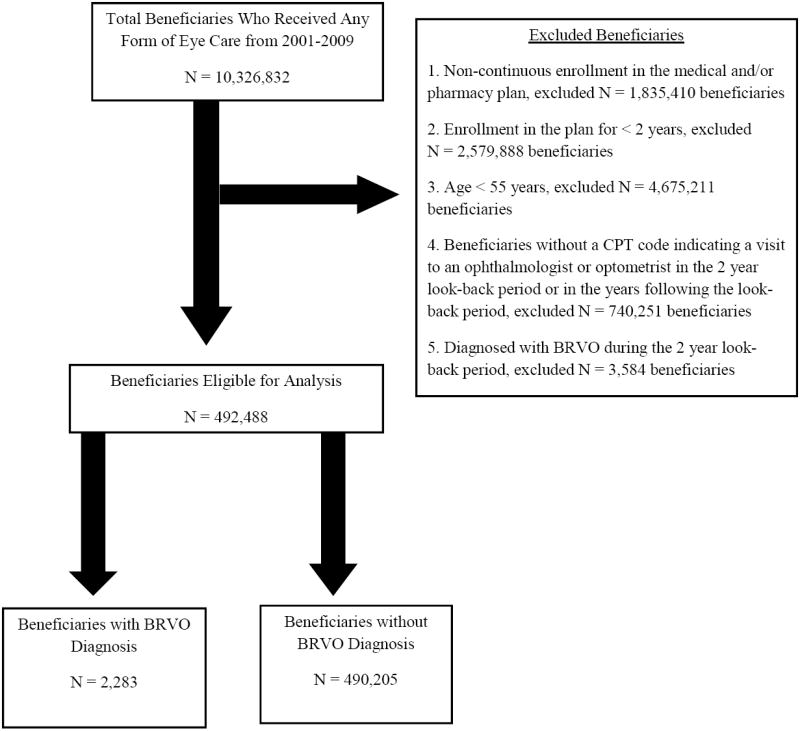
Participants: All beneficiaries age ≥55 years continuously enrolled for ≥2 years in a managed care network from 2001-2009 who had ≥2 visits to an eye care provider.
Methods: Multivariable Cox regression analyses identified sociodemographic factors, ocular and nonocular conditions associated with incident BRVO.
Main outcome measures: Hazard of incident BRVO with 95% confidence interval (CI).
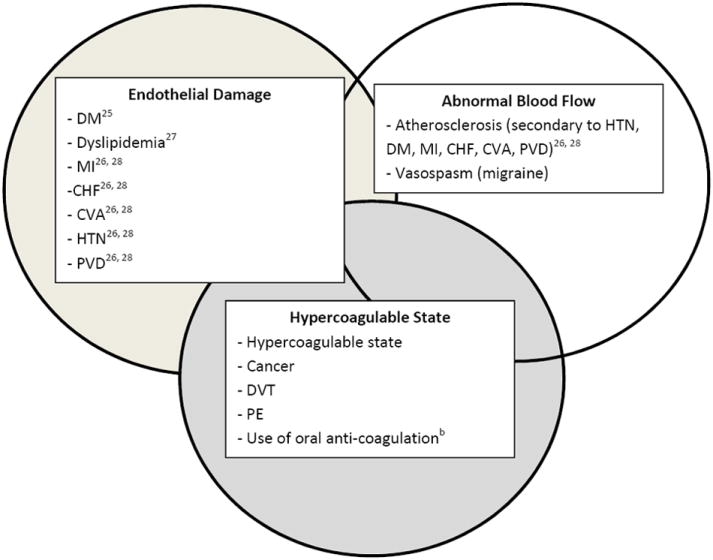
Results: Of the 492,488 enrollees who met inclusion criteria, 2283 (0.5%) developed incident BRVO. After adjustment for confounding factors, blacks (adjusted hazard ratio [aHR], 1.43; CI, 1.19-1.73; P = 0.0001) had a 43% increased hazard of BRVO relative to non-Hispanic whites. Enrollees with hypertension (HTN) alone (aHR, 1.78; CI, 1.36-2.32; P < 0.0001) or HTN along with other metabolic syndrome components (diabetes mellitus [DM] and hyperlipidemia; aHR, 1.44; CI, 1.12-1.84; P = 0.005) had an increased hazard of developing a BRVO compared with those with none of these conditions. Disease severity was important; enrollees with end-organ damage caused by HTN had a 107% increased hazard of developing BRVO compared with enrollees without HTN (aHR, 2.07; CI, 1.75-2.45; P < 0.0001). Although there was no association between DM without end-organ damage and BRVO (aHR, 0.92; CI, 0.81-1.04; P = 0.2), individuals with end-organ damage from DM had a 36% increased hazard of BRVO (aHR, 1.36; CI, 1.18-1.57; P < 0.0001) compared with those without DM. Although cerebrovascular accident was associated with an increased hazard of developing BRVO (aHR, 1.34; CI, 1.19-1.52; P < 0.0001), other diseases of the vascular system (deep venous thrombosis/pulmonary embolism, peripheral vascular disease, hypercoagulable state, myocardial infarction) or anticoagulant use did not increase the risk of BRVO (P > 0.10 for all comparisons).
Conclusions: Both HTN and end-organ damage from DM contribute to arteriosclerosis, atherosclerosis, and endothelial dysfunction, which seem to be major risk factors for BRVO. Ophthalmologists should emphasize to patients and their primary physicians the importance of effectively managing systemic medical conditions associated with BRVO.
Copyright © 2014 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicting interests regarding the material discussed in this manuscript.
Figures
References
-
- Awdeh RM, Elsing SH, Deramo VA, et al. Vision-related quality of life in persons with unilateral branch retinal vein occlusion using the 25-item National Eye Institute Visual Function Questionnaire. Br J Ophthalmol. 2010;94:319– 23. - PubMed
-
- Fekrat S, Shea AM, Hammill BG, et al. Resource use and costs of branch and central retinal vein occlusion in the elderly. Curr Med Res Opin. 2010;26:223–30. - PubMed
-
- Appiah AP, Trempe CL. Risk factors associated with branch vs. central retinal vein occlusion. Ann Ophthalmol. 1989;21:153–5. 157. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
