

The effect of care setting in the delivery of high-value colon cancer care
- PMID: 24954628
- PMCID: PMC4325980
- DOI: 10.1002/cncr.28874
The effect of care setting in the delivery of high-value colon cancer care
Abstract
Background: The effect of care setting on value of colon cancer care is unknown.
Methods: A Surveillance, Epidemiology, and End Results (SEER)-Medicare cohort study of 6544 patients aged ≥ 66 years with stage IV colon cancer (based on the American Joint Committee on Cancer staging system) who were diagnosed between 1996 and 2005 was performed. All patients were followed through December 31, 2007. Using outpatient and carrier claims, patients were assigned to a treating hospital based on the hospital affiliation of the primary oncologist. Hospitals were classified academic or nonacademic using the SEER-Medicare National Cancer Institute Hospital File.
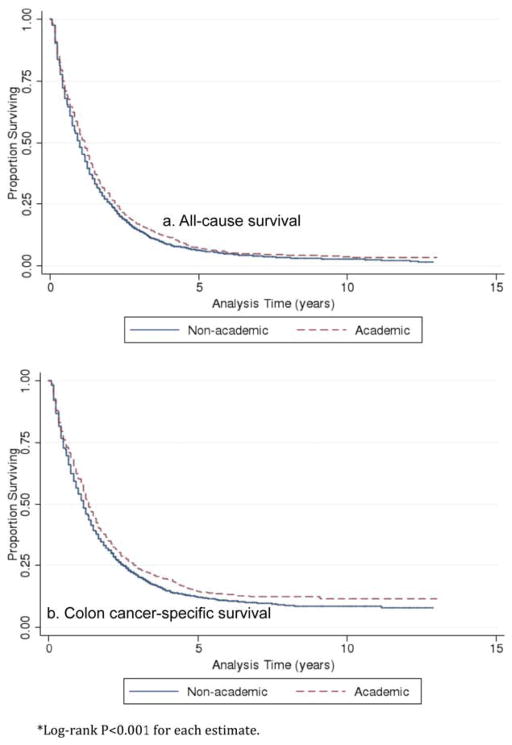
Results: Of the 6544 patients, 1605 (25%) received care from providers affiliated with academic medical centers. The unadjusted median cancer-specific survival was 16.0 months at academic medical centers versus 13.9 months at nonacademic medical centers (P < .001). After adjustment, treatment at academic hospitals remained significantly associated with a reduced risk of death from cancer (hazard ratio, 0.87; 95% confidence interval [95% CI], 0.82-0.93 [P < .001]). Adjusted mean 12-month Medicare spending was $8571 higher at academic medical centers (95% CI, $2340-$14,802; P = .007). The adjusted median cost was $1559 higher at academic medical centers; this difference was not found to be statistically significant (95% CI, -$5239 to $2122; P = .41). A small percentage of patients who received very expensive care skewed the difference in mean cost; the only statistically significant difference in adjusted costs in quantile regressions was at the 99.9th percentile of costs (P < .001).
Conclusions: Among Medicare beneficiaries with stage IV colon cancer, treatment by a provider affiliated with an academic medical center was associated with a 2 month improvement in overall survival. Except for patients in the 99.9th percentile of the cost distribution, costs at academic medical centers were not found to be significantly different from those at nonacademic medical centers.
Keywords: academic medical centers; colon cancer; cost analysis; health policy; incremental cost-effectiveness ratio; survival analysis.
© 2014 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
Dr. Pollack was supported by a National Cancer Institute grant (K07CA151910-01A1) for work performed as part of the current study.
Figures
Similar articles
-
Collaboration Between Surgeons and Medical Oncologists and Outcomes for Patients With Stage III Colon Cancer.J Oncol Pract. 2015 May;11(3):e388-97. doi: 10.1200/JOP.2014.003293. Epub 2015 Apr 14. J Oncol Pract. 2015. PMID: 25873063 Free PMC article.
-
Hospital academic status and value of care for nonmetastatic colon cancer.J Oncol Pract. 2015 May;11(3):e304-12. doi: 10.1200/JOP.2014.003137. Epub 2015 Apr 21. J Oncol Pract. 2015. PMID: 25901052 Free PMC article.
-
The Value of Continuity between Primary Care and Surgical Care in Colon Cancer.PLoS One. 2016 May 24;11(5):e0155789. doi: 10.1371/journal.pone.0155789. eCollection 2016. PLoS One. 2016. PMID: 27219454 Free PMC article.
-
Treatment disparities for disabled medicare beneficiaries with stage I non-small cell lung cancer.Arch Phys Med Rehabil. 2008 Apr;89(4):595-601. doi: 10.1016/j.apmr.2007.09.042. Arch Phys Med Rehabil. 2008. PMID: 18373987 Review.
-
Developing a liver cancer program in the nonacademic medical center.Clin Liver Dis (Hoboken). 2017 Feb 3;9(1):25-28. doi: 10.1002/cld.616. eCollection 2017 Jan. Clin Liver Dis (Hoboken). 2017. PMID: 30992952 Free PMC article. Review. No abstract available.
Cited by
-
Collaboration Between Surgeons and Medical Oncologists and Outcomes for Patients With Stage III Colon Cancer.J Oncol Pract. 2015 May;11(3):e388-97. doi: 10.1200/JOP.2014.003293. Epub 2015 Apr 14. J Oncol Pract. 2015. PMID: 25873063 Free PMC article.
-
Variation in Care of Inflammatory Bowel Diseases Patients in Crohn's and Colitis Foundation of America Partners: Role of Gastroenterologist Practice Setting in Disease Outcomes and Quality Process Measures.Inflamm Bowel Dis. 2016 Nov;22(11):2672-2677. doi: 10.1097/MIB.0000000000000933. Inflamm Bowel Dis. 2016. PMID: 27755268 Free PMC article.
-
Hospital academic status and value of care for nonmetastatic colon cancer.J Oncol Pract. 2015 May;11(3):e304-12. doi: 10.1200/JOP.2014.003137. Epub 2015 Apr 21. J Oncol Pract. 2015. PMID: 25901052 Free PMC article.
-
Impact of Sociodemographic Disparities and Insurance Status on Survival of Patients with Early-Onset Colorectal Cancer.Oncologist. 2021 Oct;26(10):e1730-e1741. doi: 10.1002/onco.13908. Epub 2021 Aug 5. Oncologist. 2021. PMID: 34288237 Free PMC article.
-
Creating a National Provider Identifier (NPI) to Unique Physician Identification Number (UPIN) Crosswalk for Medicare Data.Med Care. 2017 Dec;55(12):e113-e119. doi: 10.1097/MLR.0000000000000462. Med Care. 2017. PMID: 29135774 Free PMC article.
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- Howlader N, Noone AM, Krapcho M, Garshell J, Neyman N, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA, editors. SEER Cancer Statistics Review, 1975–2010. Bethesda, MD: National Cancer Institute; 2013.
-
- Chia SK, Speers CH, D’yachkova Y, et al. The impact of new chemotherapeutic and hormonal agents on survival in a population-based cohort of women with metastatic breast cancer. Cancer. 2007;110:973–979. - PubMed
-
- Loblaw DA, Walker-Dilks C, Winquist E, et al. Systemic therapy in men with metastatic castration-resistant prostate cancer: a systematic review. Clin Oncol (R Coll Radiol) 2013;25:406–430. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
