

Procedural and clinical utility of transulnar approach for coronary procedures following failure of radial route: Single centre experience
- PMID: 24954986
- PMCID: PMC4062755
- DOI: 10.1016/j.jsha.2014.01.003
Procedural and clinical utility of transulnar approach for coronary procedures following failure of radial route: Single centre experience
Abstract
Objectives: To assess the feasibility and safety of transulnar approach whenever transradial access fails.
Background: Radial access for coronary procedures has gained sound recognition. However, the method is not always successful.
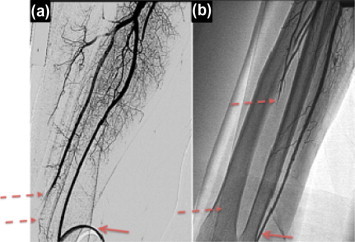
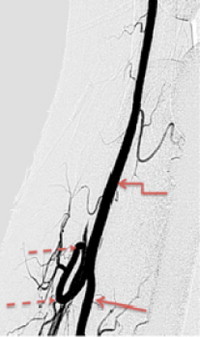
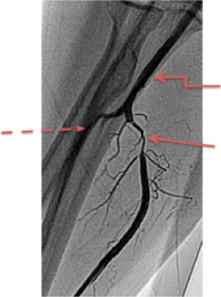
Methods: Between January 2010 and June 2013, diagnostic with or without percutaneous coronary intervention (PCI) was attempted in 2804 patients via the radial approach. Transradial approach was unsuccessful in 173 patients (6.2%) requiring crossover to either femoral (128 patients, 4.6%) or ulnar approach (45 patients, 1.6%). Patients who had undergone ulnar approach constituted our study population. Selective forearm angiography was performed after ulnar sheath placement. We documented procedural characteristics and major adverse cardio-cerebrovascular events.
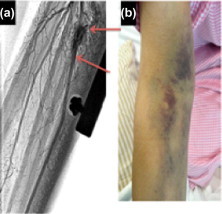
Results: Radial artery spasm was the most common cause of crossover to the ulnar approach (64.4%) followed by failure to puncture the radial artery (33.4%). Out of 45 patients (82.2%), 37 underwent successful ulnar approach. The eight failed cases (17.8%) were mainly due to absent or weak ulnar pulse (75%). PCI was performed in 17 cases (37.8%), of which 8 patients underwent emergency interventions. Complications included transient numbness, non-significant hematoma, ulnar artery perforation, and minor stroke in 15.5%, 13.3%, 2.2% and 2.2%, respectively. No major cardiac-cerebrovascular events or hand ischemia were noted.
Conclusion: Ulnar approach for coronary diagnostic or intervention procedures is a feasible alternative whenever radial route fails. It circumvents crossover to the femoral approach. Our study confirms satisfactory success rate of ulnar access in the presence of adequate ulnar pulse intensity and within acceptable rates of complications.
Keywords: Alternative; Coronary procedures; Feasible; Femoral approach; MACCE; Radial; Ulnar.
Figures


Similar articles
-
Feasibility and Safety of Ipsilateral Ulnar Access in Cases of Impossibility or Failure of Radial Access for Coronary Angiography or Percutaneous Coronary Intervention.J Invasive Cardiol. 2022 Feb;34(2):E92-E97. doi: 10.25270/jic/21.00138. Epub 2022 Jan 16. J Invasive Cardiol. 2022. PMID: 35037897
-
Safety and feasibility of transulnar catheterization when ipsilateral radial access is not available.Catheter Cardiovasc Interv. 2014 Jan 1;83(1):E51-60. doi: 10.1002/ccd.25123. Epub 2013 Aug 5. Catheter Cardiovasc Interv. 2014. PMID: 23832623
-
Transulnar approach as an alternative access site for coronary invasive procedures after transradial approach failure.Am Heart J. 2012 Oct;164(4):462-7. doi: 10.1016/j.ahj.2012.08.001. Am Heart J. 2012. PMID: 23067902
-
Transulnar cardiac catheterization and percutaneous coronary intervention: techniques, transradial comparisons, anatomical considerations, and comprehensive literature review.Catheter Cardiovasc Interv. 2017 Dec 1;90(7):1126-1134. doi: 10.1002/ccd.27220. Epub 2017 Aug 2. Catheter Cardiovasc Interv. 2017. PMID: 28766859 Review.
-
Transulnar versus transradial access for coronary angiography or percutaneous coronary intervention: A meta-analysis of randomized controlled trials.Catheter Cardiovasc Interv. 2016 Apr;87(5):857-65. doi: 10.1002/ccd.26221. Epub 2015 Sep 2. Catheter Cardiovasc Interv. 2016. PMID: 26332022 Review.
Cited by
-
Percutaneous trans-ulnar versus trans-radial arterial approach for coronary angiography and angioplasty, a preliminary experience at an Egyptian cardiology center.Egypt Heart J. 2020 Sep 11;72(1):60. doi: 10.1186/s43044-020-00089-7. Egypt Heart J. 2020. PMID: 32915325 Free PMC article.
-
Distal accesses in the hand (two novel techniques) for percutaneous coronary angiography and intervention.ARYA Atheroscler. 2018 Mar;14(2):95-100. doi: 10.22122/arya.v14i2.1743. ARYA Atheroscler. 2018. PMID: 30108641 Free PMC article.
-
Transulnar versus transradial approach for coronary angiography and angioplasty: Considering their complications.ARYA Atheroscler. 2018 May;14(3):128-131. doi: 10.22122/arya.v14i3.1586. ARYA Atheroscler. 2018. PMID: 30349575 Free PMC article.
References
-
- Jolly S.S., Yusuf S., Cairns J., Niemelä K., Xavier D., Widimsky P. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomized, parallel group, multicenter trial. Lancet. 2011;377(9775):1409–1420. - PubMed
-
- Kiemeneij F., Laarman G.J., Odekerken D., Slagboom T., van der Wieken R. A randomized comparison of percutaneous transluminal coronary angioplasty by the radial, brachial and femoral approaches: the access study. J Am Coll Cardiol. 1997;29(6):1269–1275. - PubMed
-
- Louvard Y., Lefèvre T., Allain A., Morice M. Coronary angiography through the radial or the femoral approach: the CARAFE study. Catheter Cardiovasc Interv. 2001;52(2):181–187. - PubMed
-
- Biondi-Zoccai G., Sciahbasi A., Bodí V., Fernández-Portales J., Kanei Y., Romagnoli E. Right versus left radial artery access for coronary procedures: an international collaborative systematic review and meta-analysis including 5 randomized trials and 3210 patients. Int J Cardiol. 2013;166(3):621–626. - PubMed
-
- Valsecchi O., Vassileva A., Musumeci G., Rossini R., Tespili M., Guagliumi G. Failure of transradial approach during coronary interventions: anatomic considerations. Catheter Cardiovasc Interv. 2006;67(6):870–878. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
