

Outpatient management of heart failure in the United States, 2006-2008
- PMID: 24955039
- PMCID: PMC4060338
- DOI: 10.14503/THIJ-12-2947
Outpatient management of heart failure in the United States, 2006-2008
Abstract
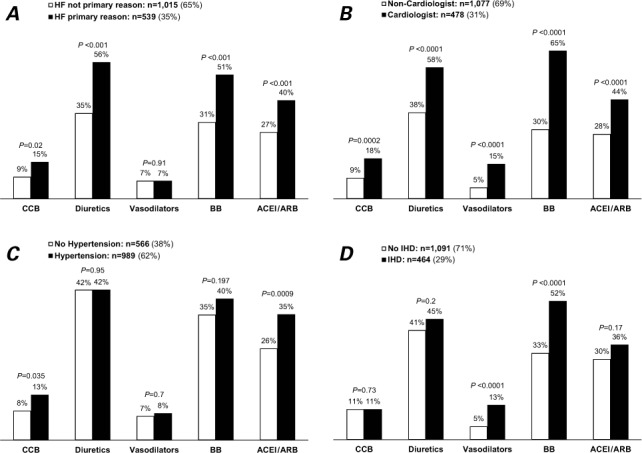
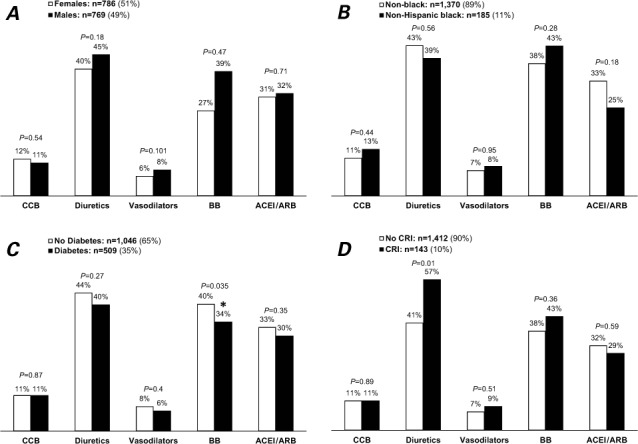
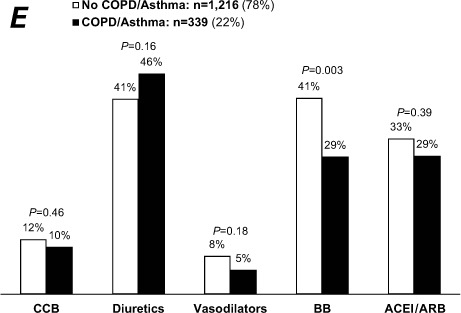
Better outpatient management of heart failure might improve outcomes and reduce the number of rehospitalizations. This study describes recent outpatient heart-failure management in the United States. We analyzed data from the National Ambulatory Medical Care Survey of 2006-2008, a multistage random sampling of non-Federal physician offices and hospital outpatient departments. Annually, 1.7% of all outpatient visits were for heart failure (51% females and 77% non-Hispanic whites; mean age, 73 ± 0.5 yr). Typical comorbidities were hypertension (62%), hyperlipidemia (36%), diabetes mellitus (35%), and ischemic heart disease (29%). Body weight and blood pressure were recorded in about 80% of visits, and health education was given in about 40%. The percentage of patients taking β-blockers was 38%; the percentage taking angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (ACEI/ARBs) was 32%. Medication usage did not differ significantly by race or sex. In multivariate-adjusted logistic regression models, a visit to a cardiologist, hypertension, heart failure as a primary reason for the visit, and a visit duration longer than 15 minutes were positively associated with ACEI/ARB use; and a visit to a cardiologist, heart failure as a primary reason for the visit, the presence of ischemic heart disease, and visit duration longer than 15 minutes were positively associated with β-blocker use. Chronic obstructive pulmonary disease was negatively associated with β-blocker use. Approximately 1% of heart-failure visits resulted in hospitalization. In outpatient heart-failure management, gaps that might warrant attention include suboptimal health education and low usage rates of medications, specifically ACEI/ARBs and β-blockers.
Keywords: Ambulatory care/standards; cardiovascular agents/therapeutic use; clinical trials as topic; comprehensive health care; drug utilization/statistics & numerical data; health care surveys; heart failure/drug therapy/economics/epidemiology/prevention & control; office visits/statistics & numerical data/trends/utilization; outcome assessment (health care)/trends; quality assurance, health care.
Figures
Similar articles
-
Prescribing patterns of evidence-based heart failure pharmacotherapy and outcomes in the ASIAN-HF registry: a cohort study.Lancet Glob Health. 2018 Sep;6(9):e1008-e1018. doi: 10.1016/S2214-109X(18)30306-1. Lancet Glob Health. 2018. PMID: 30103979
-
Use of guideline-recommended therapies for heart failure in the Medicare population.Clin Cardiol. 2010 Jul;33(7):400-5. doi: 10.1002/clc.20760. Clin Cardiol. 2010. PMID: 20641116 Free PMC article.
-
Lack of improvement in outpatient management of congestive heart failure in the United States.Arch Intern Med. 2010 Aug 9;170(15):1399-400. doi: 10.1001/archinternmed.2010.270. Arch Intern Med. 2010. PMID: 20696970 Free PMC article. No abstract available.
-
Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, 1997.Vital Health Stat 13. 1999 Nov;(143):i-iv, 1-39. Vital Health Stat 13. 1999. PMID: 10633576 Review.
-
Economic Issues in Heart Failure in the United States.J Card Fail. 2022 Mar;28(3):453-466. doi: 10.1016/j.cardfail.2021.12.017. Epub 2022 Jan 24. J Card Fail. 2022. PMID: 35085762 Free PMC article. Review.
Cited by
-
Chronic Heart Failure Clinical Practice Guidelines' Class 1-A Pharmacologic Recommendations: Start-to-End Synergistic Drug Therapy?ASEAN Heart J. 2016 Mar 8;24(1):4. doi: 10.7603/s40602-016-0004-5. eCollection 2016 Mar. ASEAN Heart J. 2016. PMID: 27054142 Free PMC article.
-
Treatment Initiation Patterns, Modifications, and Medication Adherence Among Newly Diagnosed Heart Failure Patients: A Retrospective Claims Database Analysis.J Manag Care Spec Pharm. 2016 May;22(5):561-71. doi: 10.18553/jmcp.2016.22.5.561. J Manag Care Spec Pharm. 2016. PMID: 27123917 Free PMC article.
-
Association of Patient and Primary Care Provider Factors with Outpatient COPD Care Quality.Chronic Obstr Pulm Dis. 2022 Jan 27;9(1):55-67. doi: 10.15326/jcopdf.2021.0232. Chronic Obstr Pulm Dis. 2022. PMID: 34915603 Free PMC article.
-
Quality of medical care for persons with serious mental illness: A comprehensive review.Schizophr Res. 2015 Jul;165(2-3):227-35. doi: 10.1016/j.schres.2015.04.010. Epub 2015 Apr 27. Schizophr Res. 2015. PMID: 25936686 Free PMC article. Review.
-
The Relationship between Nocturnal Dipping Status, Morning Blood Pressure Surge, and Hospital Admissions in Patients with Systolic Heart Failure.Arq Bras Cardiol. 2023 Sep 18;120(9):e20220932. doi: 10.36660/abc.20220932. eCollection 2023. Arq Bras Cardiol. 2023. PMID: 37729291 Free PMC article. English, Portuguese.
References
-
- Massie BM, Shah NB. Evolving trends in the epidemiologic factors of heart failure: rationale for preventive strategies and comprehensive disease management. Am Heart J. 1997;133(6):703–12. - PubMed
-
- Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM et al. Heart disease and stroke statistics–2011 update: a report from the American Heart Association [published errata appear in Circulation 2011;123(6):e240 and Circulation 2011;124(16):e246] Circulation. 2011;123(4):e18–e209. - PMC - PubMed
-
- Kosiborod M, Lichtman JH, Heidenreich PA, Normand SL, Wang Y, Brass LM, Krumholz HM. National trends in outcomes among elderly patients with heart failure. Am J Med. 2006;119(7):616.e1–7. - PubMed
-
- Oddone EZ, Weinberger M, Horner M, Mengel C, Goldstein F, Ginier P et al. Classifying general medicine readmissions. Are they preventable? Veterans Affairs Cooperative Studies in Health Services Group on Primary Care and Hospital Readmissions. J Gen Intern Med. 1996;11(10):597–607. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
