

Do the morphological features of walled off pancreatic necrosis on endoscopic ultrasound determine the outcome of endoscopic transmural drainage?
- PMID: 24955341
- PMCID: PMC4064159
- DOI: 10.4103/2303-9027.131039
Do the morphological features of walled off pancreatic necrosis on endoscopic ultrasound determine the outcome of endoscopic transmural drainage?
Abstract
Background and objective: Endoscopic transmural drainage is an effective, but technically demanding treatment modality for walled off pancreatic necrosis (WOPN). The factors that determine the outcome of endoscopic treatment for WOPN have been infrequently studied. We aim to retrospectively correlate the morphological features of WOPN on endoscopic ultrasound (EUS) with the outcome of endoscopic transmural drainage.
Patients and methods: Over the last 3 years, 43 patients (36 males; mean age 36.04 ± 10.06 years) with symptomatic WOPN were treated by an attempted endoscopic drainage. The correlation between the morphological features of WOPN and the type of treatment offered as well as the number of endoscopic procedures undergone by the patient was assessed.
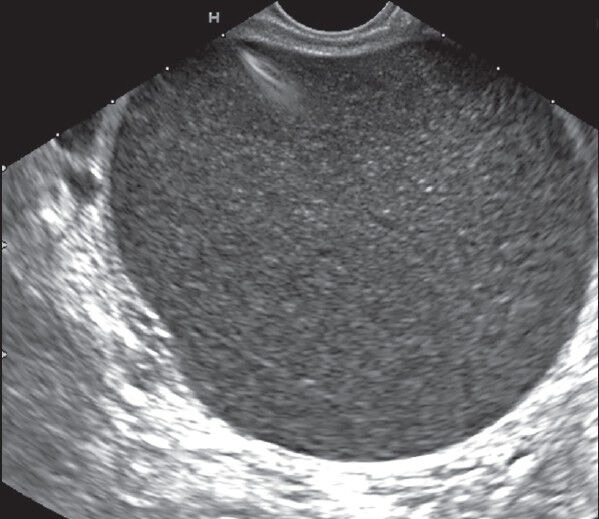
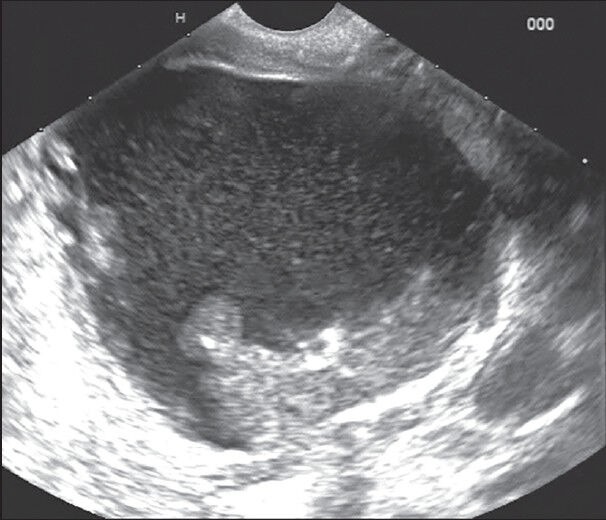
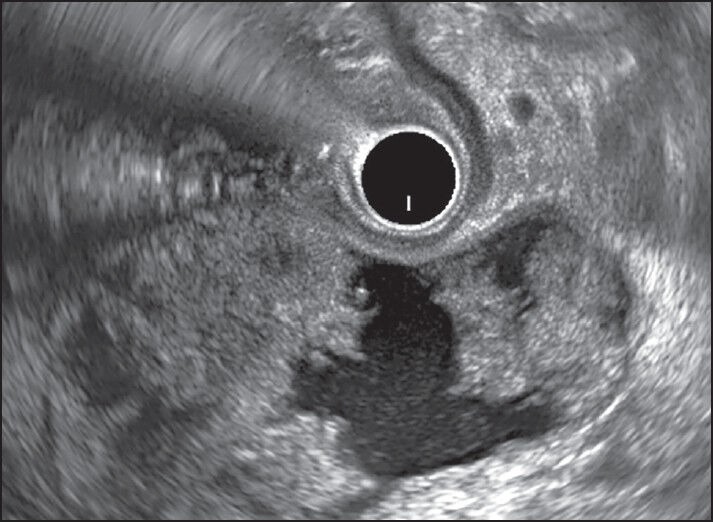
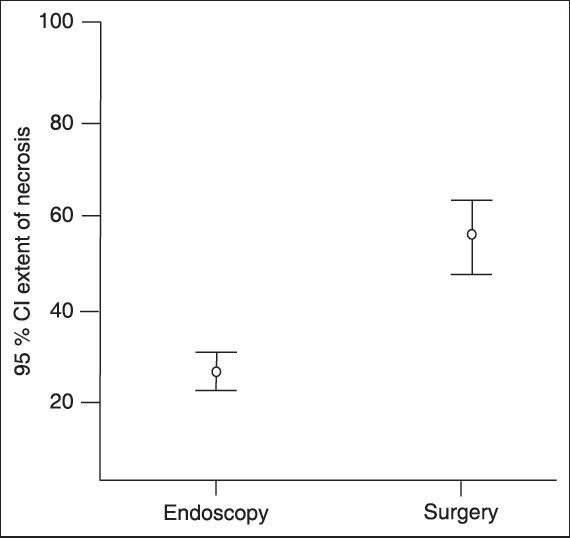
Results: The mean size of WOPN was 9.95 ± 2.75 cm with <10%, 10-40% and >40% solid debris being present in 6, 33, and 4 patients, respectively. Patients with <10% necrotic debris needed only single session of endoscopic drainage, whereas patients with 10-40% solid debris needed two or more sessions. Patients with >40% solid debris either needed direct endoscopic debridement or surgical necrosectomy. The extent of necrosis correlated significantly (r = 0.703, P < 0.001) with the type of treatment received by the patient. With increasing size of the collection (r = 0.320, P = 0.047) and the amount of the solid debris (r = 0.800, P < 0.001), there was a significant increase in the number of endoscopic procedures required for successful outcome by the patient.
Conclusions: The morphological features of WOPN on EUS have important therapeutic implications with collections having large size and more solid debris needing more aggressive therapeutic method for the successful outcome.
Keywords: Acute pancreatitis; computed tomography; endoscopic ultrasound; walled off pancreatic necrosis.
Conflict of interest statement
Figures
References
-
- Rana SS, Bhasin DK, Rao C, et al. Non-fluoroscopic endoscopic ultrasound-guided transmural drainage of symptomatic non-bulging walled-off pancreatic necrosis. Dig Endosc. 2013;25:47–52. - PubMed
-
- Seewald S, Groth S, Omar S, et al. Aggressive endoscopic therapy for pancreatic necrosis and pancreatic abscess: A new safe and effective treatment algorithm (videos) Gastrointest Endosc. 2005;62:92–100. - PubMed
-
- Charnley RM, Lochan R, Gray H, et al. Endoscopic necrosectomy as primary therapy in the management of infected pancreatic necrosis. Endoscopy. 2006;38:925–8. - PubMed
-
- Seifert H, Biermer M, Schmitt W, et al. Transluminal endoscopic necrosectomy after acute pancreatitis: A multicentre study with long-term follow-up (the GEPARD Study) Gut. 2009;58:1260–6. - PubMed
-
- Gardner TB, Chahal P, Papachristou GI, et al. A comparison of direct endoscopic necrosectomy with transmural endoscopic drainage for the treatment of walled-off pancreatic necrosis. Gastrointest Endosc. 2009;69:1085–94. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
