

Liver dysfunction assessed by model for end-stage liver disease excluding INR (MELD-XI) scoring system predicts adverse prognosis in heart failure
- PMID: 24955578
- PMCID: PMC4067358
- DOI: 10.1371/journal.pone.0100618
Liver dysfunction assessed by model for end-stage liver disease excluding INR (MELD-XI) scoring system predicts adverse prognosis in heart failure
Abstract
Aims: Liver dysfunction due to heart failure (HF) is often referred to as cardiac or congestive hepatopathy. The composite Model for End-Stage Liver Disease excluding INR (MELD-XI) is a robust scoring system of liver function, and a high score is associated with poor prognosis in advanced HF patients with a heart transplantation and/or ventricular assist device. However, the impact of MELD-XI on the prognosis of HF patients in general remains unclear.
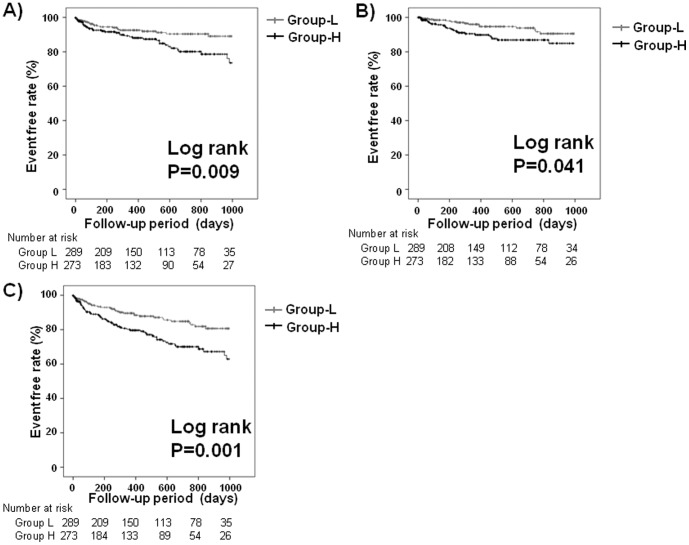
Methods and results: We retrospectively analyzed 562 patients who were admitted to our hospital for the treatment of decompensated HF. A MELD-XI score was graded, and patients were divided into two groups based on the median value of MELD-XI score: Group L (MELD-XI <10, n = 289) and Group H (MELD-XI ≥10, n = 273). We compared all-cause mortality and echocardiographic findings between the two groups. In the follow-up period (mean 471 days), 104 deaths (62 cardiac deaths and 42 non-cardiac deaths) were observed. The event (cardiac death, non-cardiac death, all-cause death)-free rate was significantly higher in group L than in group H (logrank P<0.05, respectively). In the Cox proportional hazard analysis, a high MELD-XI score was found to be an independent predictor of cardiac deaths and all-cause mortality in HF patients. Regarding echocardiographic parameters, right atrial and ventricular areas, inferior vena cava diameter, and systolic pulmonary artery pressure were higher in group H than in group L (P<0.05, respectively).
Conclusions: The MELD-XI scoring system, a marker of liver function, can identify high-risk patients with right heart volume overload, higher pulmonary arterial pressure and multiple organ failure associated with HF.
Conflict of interest statement
Figures
References
-
- Poelzl G, Ess M, Mussner-Seeber C, Pachinger O, Frick M, et al. (2012) Liver dysfunction in chronic heart failure: prevalence, characteristics and prognostic significance. Eur J Clin Invest 42: 153–163. - PubMed
-
- Allen LA, Felker GM, Pocock S, McMurray JJ, Pfeffer MA, et al. (2009) Liver function abnormalities and outcome in patients with chronic heart failure: data from the Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) program. Eur J Heart Fail 11: 170–177. - PMC - PubMed
-
- Batin P, Wickens M, McEntegart D, Fullwood L, Cowley AJ (1995) The importance of abnormalities of liver function tests in predicting mortality in chronic heart failure. Eur Heart J 16: 1613–1618. - PubMed
-
- Shinagawa H, Inomata T, Koitabashi T, Nakano H, Takeuchi I, et al. (2008) Prognostic significance of increased serum bilirubin levels coincident with cardiac decompensation in chronic heart failure. Circ J 72: 364–369. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
