

High-throughput sequencing analysis of post-liver transplantation HCV E2 glycoprotein evolution in the presence and absence of neutralizing monoclonal antibody
- PMID: 24956119
- PMCID: PMC4067308
- DOI: 10.1371/journal.pone.0100325
High-throughput sequencing analysis of post-liver transplantation HCV E2 glycoprotein evolution in the presence and absence of neutralizing monoclonal antibody
Abstract
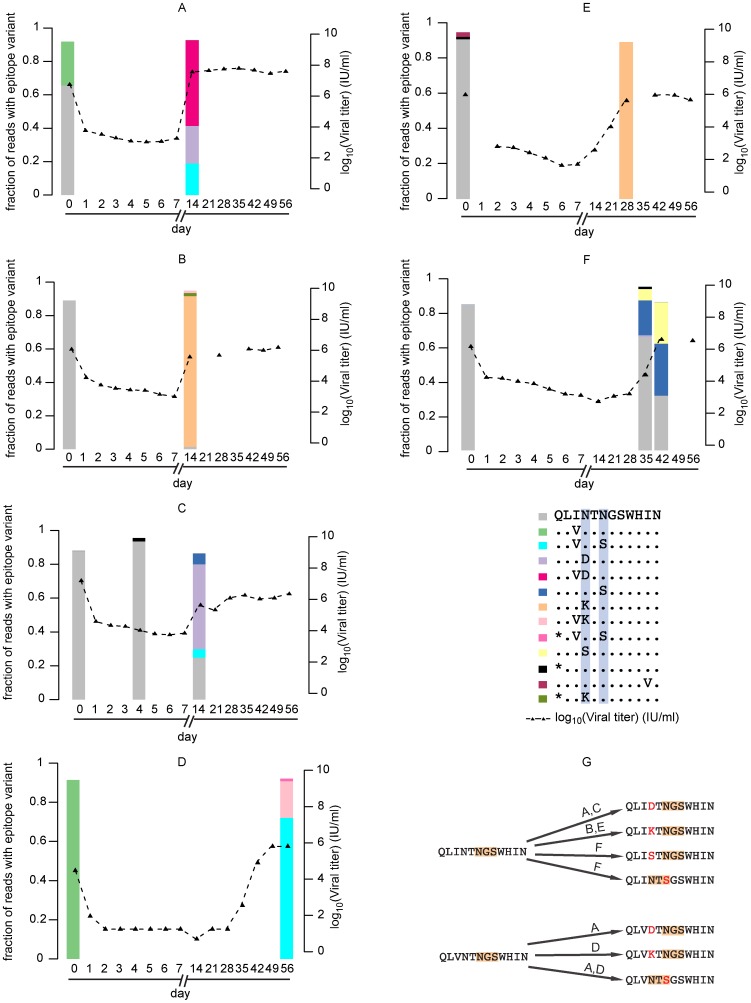
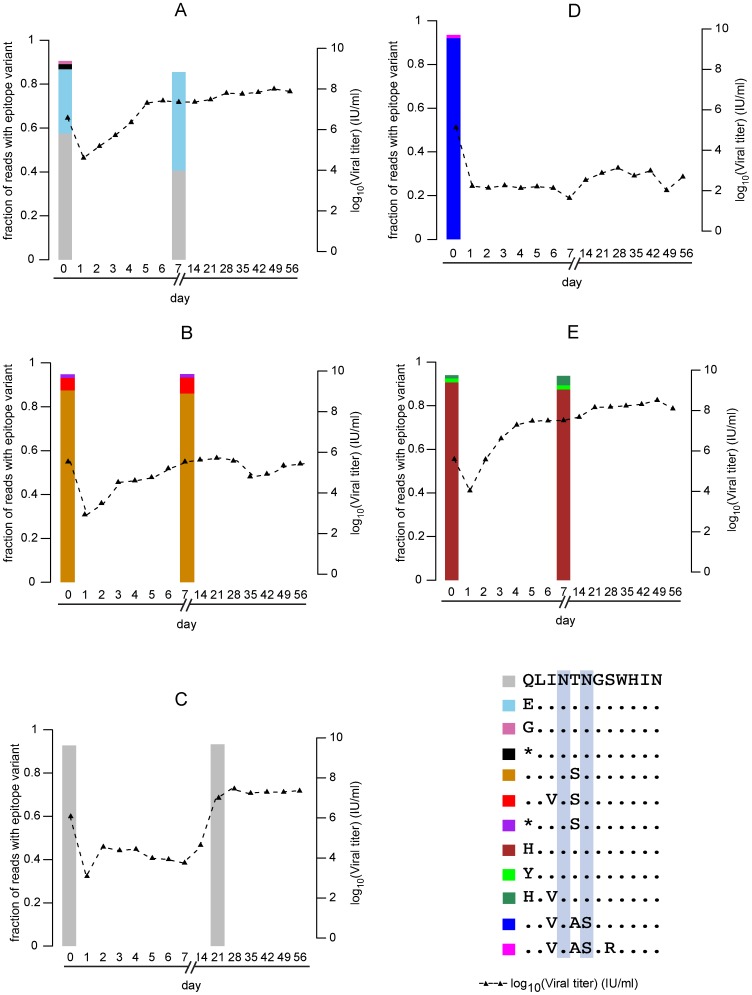
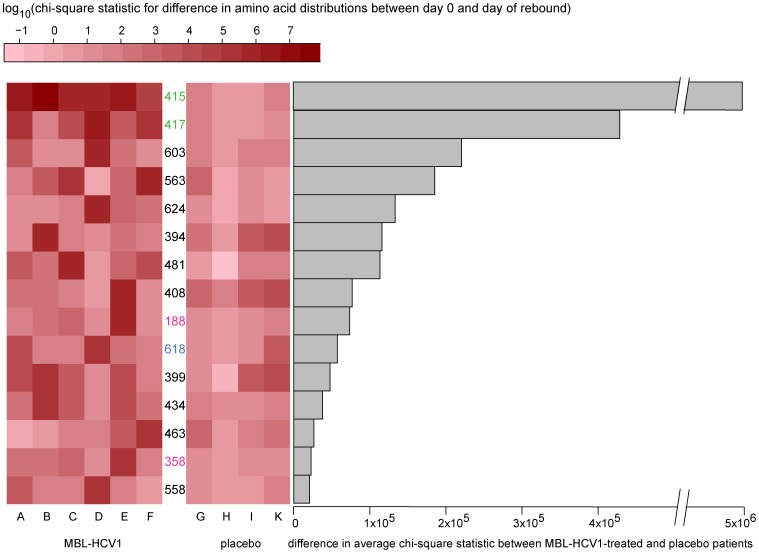
Chronic hepatitis C virus (HCV) infection is the most common cause of end-stage liver disease, often leading to liver transplantation, in which case circulating virions typically infect the transplanted liver within hours and viral concentrations can quickly exceed pre-transplant levels. MBL-HCV1 is a fully human monoclonal antibody recognizing a linear epitope of the HCV E2 envelope glycoprotein (amino acids 412-423). The ability of MBL-HCV1 to prevent HCV recurrence after liver transplantation was investigated in a phase 2 randomized clinical trial evaluating six MBL-HCV1-treated subjects and five placebo-treated subjects. MBL-HCV1 treatment significantly delayed time to viral rebound compared with placebo treatment. Here we report results from high-throughput sequencing on the serum of each of the eleven enrolled subjects prior to liver transplantation and after viral rebound. We further sequenced the sera of the MBL-HCV1-treated subjects at various interim time points to study the evolution of antibody-resistant viral variants. We detected mutations at one of two positions within the antibody epitope--mutations of N at position 415 to D, K or S, or mutation of N at position 417 to S. It has been previously reported that N415 is not glycosylated in the wild-type E2 protein, but N417S can lead to glycosylation at position 415. Thus N415 is a key position for antibody recognition and the only routes we identified for viral escape, within the constraints of HCV fitness in vivo, involve mutating or glycosylating this position. Evaluation of mutations along the entire E1 and E2 proteins revealed additional positions that changed moderately before and after MBL-HCV1 treatment for subsets of the six subjects, yet underscored the relative importance of position 415 in MBL-HCV1 resistance.
Conflict of interest statement
Figures
References
-
- Kim WR, Stock PG, Smith JM, Heimbach JK, Skeans MA, et al. (2013) OPTN/SRTR 2011 Annual Data Report: Liver. American Journal of Transplantation 13: 73. - PubMed
-
- Garcia-Retortillo M, Forns X, Feliu A, Moitinho E, Costa J, et al. (2002) Hepatitis C virus kinetics during and immediately after liver transplantation. Hepatology 35: 680–687. - PubMed
-
- Powers KA, Ribeiro RM, Patel K, Pianko S, Nyberg L, et al. (2006) Kinetics of hepatitis C virus reinfection after liver transplantation. Liver Transpl 12: 207–216. - PubMed
-
- Crespo G, Marino Z, Navasa M, Forns X (2012) Viral hepatitis in liver transplantation. Gastroenterology 142: 1373–1383 e1371. - PubMed
-
- Gallegos-Orozco JF, Yosephy A, Noble B, Aqel BA, Byrne TJ, et al. (2009) Natural history of post-liver transplantation hepatitis C: A review of factors that may influence its course. Liver Transpl 15: 1872–1881. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
