

Sex-dependent influence of endogenous estrogen in pulmonary hypertension
- PMID: 24956156
- PMCID: PMC4214128
- DOI: 10.1164/rccm.201403-0483OC
Sex-dependent influence of endogenous estrogen in pulmonary hypertension
Abstract
Rationale: The incidence of pulmonary arterial hypertension is greater in women, suggesting estrogens may play a role in the disease pathogenesis. Experimentally, in males, exogenously administered estrogen can protect against pulmonary hypertension (PH). However, in models that display female susceptibility, estrogens may play a causative role.
Objectives: To clarify the influence of endogenous estrogen and sex in PH and assess the therapeutic potential of a clinically available aromatase inhibitor.
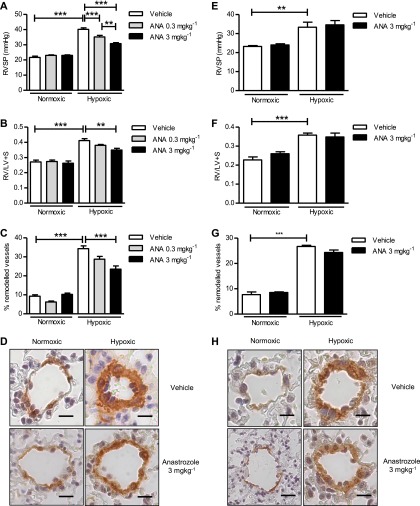
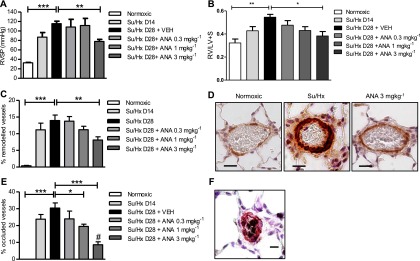
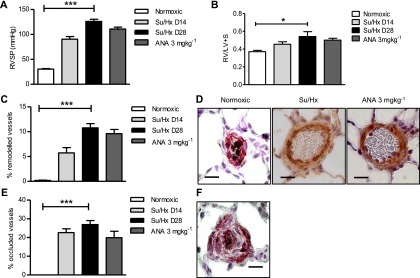
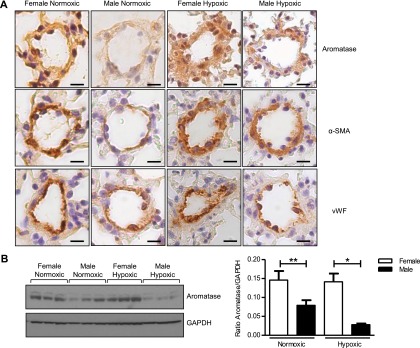
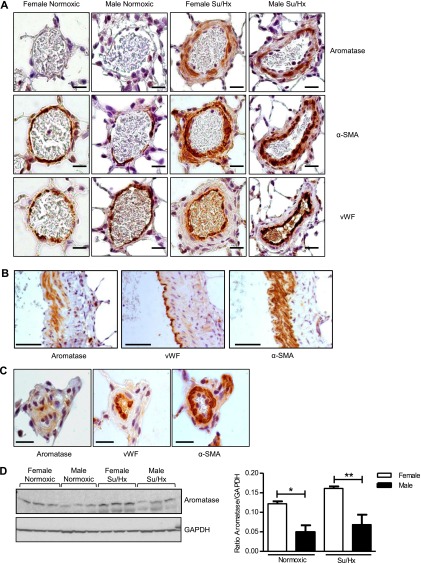
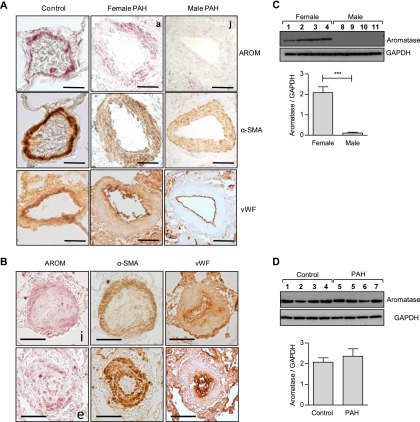
Methods: We interrogated the effect of reduced endogenous estrogen in males and females using the aromatase inhibitor, anastrozole, in two models of PH: the hypoxic mouse and Sugen 5416/hypoxic rat. We also determined the effects of sex on pulmonary expression of aromatase in these models and in lungs from patients with pulmonary arterial hypertension.
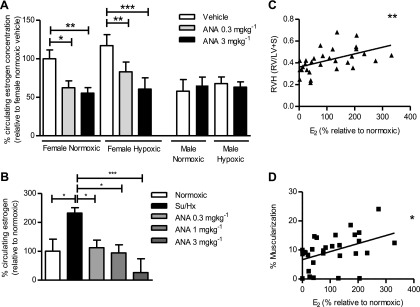
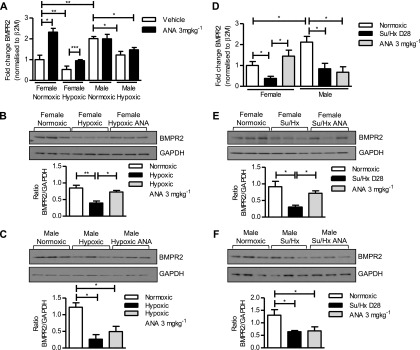
Measurements and main results: Anastrozole attenuated PH in both models studied, but only in females. To verify this effect was caused by reduced estrogenic activity we confirmed that in hypoxic mice inhibition of estrogen receptor α also has a therapeutic effect specifically in females. Female rodent lung displays increased aromatase and decreased bone morphogenetic protein receptor 2 and Id1 expression compared with male. Anastrozole treatment reversed the impaired bone morphogenetic protein receptor 2 pathway in females. Increased aromatase expression was also detected in female human pulmonary artery smooth muscle cells compared with male.
Conclusions: The unique phenotype of female pulmonary arteries facilitates the therapeutic effects of anastrozole in experimental PH confirming a role for endogenous estrogen in the disease pathogenesis in females and suggests aromatase inhibitors may have therapeutic potential.
Keywords: estrogen; pulmonary hypertension; sex.
Figures
References
-
- Shapiro S, Traiger GL, Turner M, McGoon MD, Wason P, Barst RJ. Sex differences in the diagnosis, treatment, and outcome of patients with pulmonary arterial hypertension enrolled in the registry to evaluate early and long-term pulmonary arterial hypertension disease management. Chest. 2012;141:363–373. - PubMed
-
- McGoon MD, Benza RL, Escribano-Subias P, Jiang X, Miller DP, Peacock AJ, Pepke-Zaba J, Pulido T, Rich S, Rosenkranz S, et al. Pulmonary arterial hypertension: epidemiology and registries. J Am Coll Cardiol. 2013;62(Suppl. 25):D51–D59. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
