

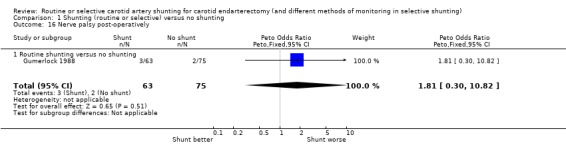
Routine or selective carotid artery shunting for carotid endarterectomy (and different methods of monitoring in selective shunting)
- PMID: 24956204
- PMCID: PMC7032624
- DOI: 10.1002/14651858.CD000190.pub3
Routine or selective carotid artery shunting for carotid endarterectomy (and different methods of monitoring in selective shunting)
Update in
-
Routine or selective carotid artery shunting for carotid endarterectomy (and different methods of monitoring in selective shunting).Cochrane Database Syst Rev. 2022 Jun 22;6(6):CD000190. doi: 10.1002/14651858.CD000190.pub4. Cochrane Database Syst Rev. 2022. PMID: 35731671 Free PMC article.
Abstract
Background: Temporary interruption of cerebral blood flow during carotid endarterectomy can be avoided by using a shunt across the clamped section of the carotid artery. This may improve outcome. This is an update of a Cochrane review originally published in 1996 and previously updated in 2009.
Objectives: To assess the effect of routine versus selective or no shunting during carotid endarterectomy, and to assess the best method for selecting people for shunting.
Search methods: We searched the Cochrane Stroke Group Trials Register (last searched August 2013), the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library, 2013, Issue 8), MEDLINE (1966 to August 2013), EMBASE (1980 to August 2013) and Index to Scientific and Technical Proceedings (1980 to August 2013). We handsearched journals and conference proceedings, checked reference lists, and contacted experts in the field.
Selection criteria: Randomised and quasi-randomised trials of routine shunting compared with no shunting or selective shunting, and trials that compared different shunting policies in people undergoing carotid endarterectomy.
Data collection and analysis: Three review authors independently performed the searches and applied the inclusion criteria. For this update, we identified two new relevant randomised controlled trials.
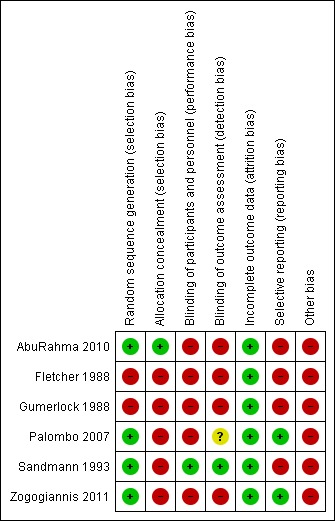
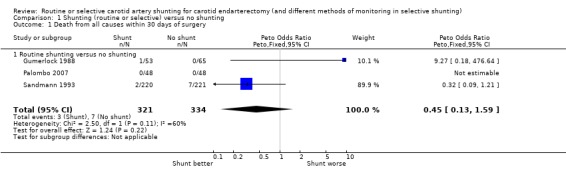
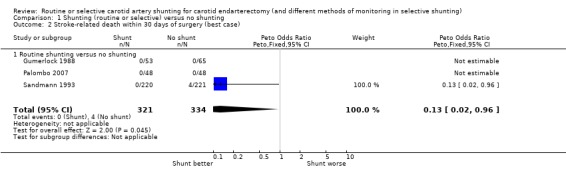
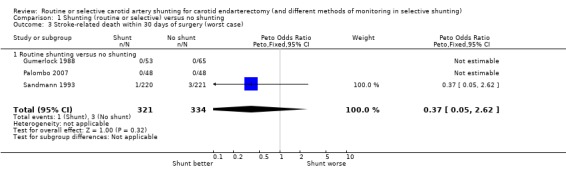
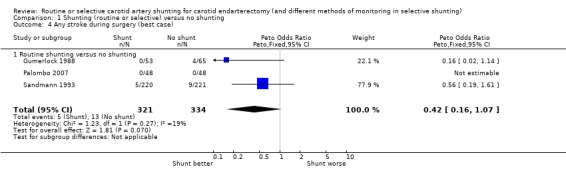
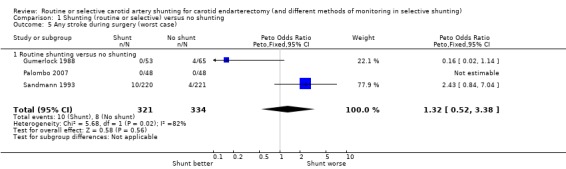
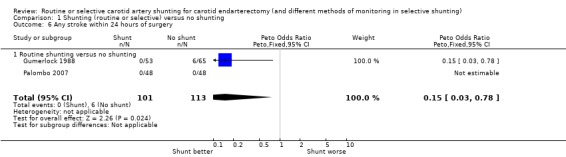
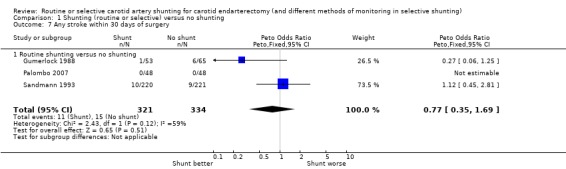
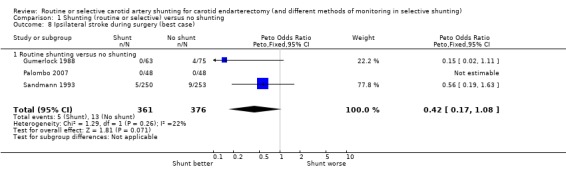
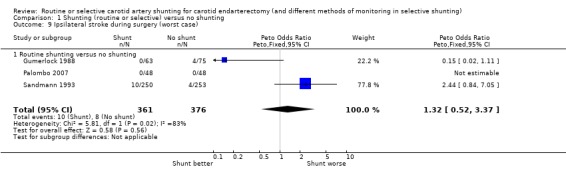
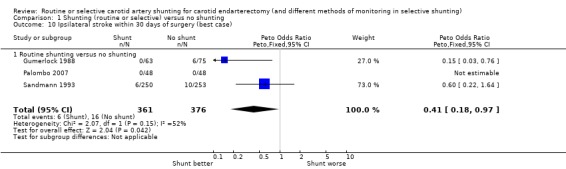
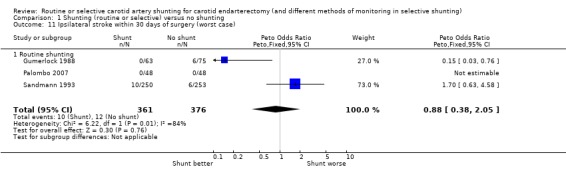
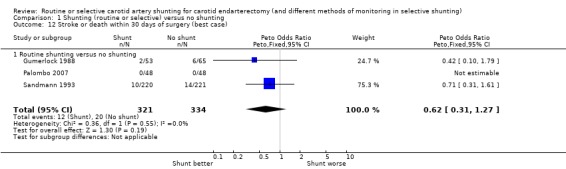
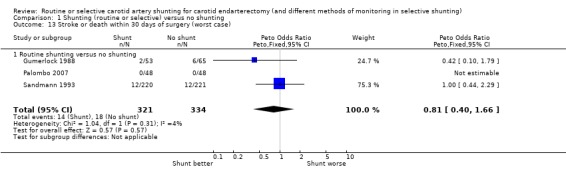
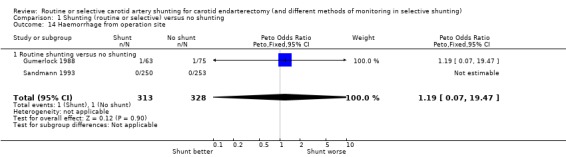
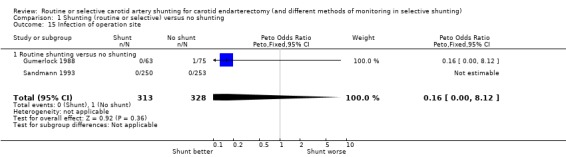
Main results: We included six trials involving 1270 participants in the review: three trials involving 686 participants compared routine shunting with no shunting, one trial involving 200 participants compared routine shunting with selective shunting, one trial involving 253 participants compared selective shunting with and without near-infrared refractory spectroscopy monitoring, and the other trial involving 131 participants compared shunting with a combination of electroencephalographic and carotid pressure measurement with shunting by carotid pressure measurement alone. In general, reporting of methodology in the included studies was poor. For most studies, the blinding of outcome assessors and the report of prespecified outcomes were unclear. For routine versus no shunting, there was no significant difference in the rate of all stroke, ipsilateral stroke or death up to 30 days after surgery, although data were limited. No significant difference was found between the groups in terms of postoperative neurological deficit between selective shunting with and without near-infrared refractory spectroscopy monitoring, However, this analysis was inadequately powered to reliably detect the effect. There was no significant difference between the risk of ipsilateral stroke in participants selected for shunting with the combination of electroencephalographic and carotid pressure assessment compared with pressure assessment alone, although again the data were limited.
Authors' conclusions: This review concluded that the data available were too limited to either support or refute the use of routine or selective shunting in carotid endarterectomy. Large scale randomised trials of routine shunting versus selective shunting are required. No method of monitoring in selective shunting has been shown to produce better outcomes.
Conflict of interest statement
None known.
Figures
Update of
-
Routine or selective carotid artery shunting for carotid endarterectomy (and different methods of monitoring in selective shunting).Cochrane Database Syst Rev. 2009 Oct 7;(4):CD000190. doi: 10.1002/14651858.CD000190.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2014 Jun 23;(6):CD000190. doi: 10.1002/14651858.CD000190.pub3. PMID: 19821268 Updated.
References
References to studies included in this review
AbuRahma 2010 {published data only}
-
- Aburahma AF, Stone PA, Hass SM, Dean LS, Habib J, Keiffer T, et al. Prospective randomized trial of routine versus selective shunting in carotid endarterectomy based on stump pressure. Journal of Vascular Surgery 2010;51:1133‐8. - PubMed
Fletcher 1988 {published data only}
-
- Fletcher JP, Morris JGL, Little JM, Kershaw LZ. EEG monitoring during carotid endarterectomy. Australian and New Zealand Journal of Surgery 1988;58:285‐8. - PubMed
Gumerlock 1988 {published and unpublished data}
-
- Gumerlock MK, Neuwelt EA. Carotid endarterectomy: to shunt or not to shunt. Stroke 1988;19:1485‐90. - PubMed
Palombo 2007 {published data only}
-
- Palombo D, Lucertini G, Mambrini S, Zettin M. Subtle cerebral damage after shunting vs non shunting during carotid endarterectomy. European Journal of Vascular and Endovascular Surgery 2007;34:546‐51. - PubMed
Sandmann 1993 {published and unpublished data}
-
- Sandmann W, Kolvenbach R, Willeke F. Risks and benefits of shunting in carotid endarterectomy. Stroke 1993;24:1098. - PubMed
-
- Sandmann W, Willeke F, Kovenbach R, Benecke R, Godehardt E. To shunt or not to shunt: the definite answer with a randomized study. In: Veith FJ editor(s). Current Critical Problems in Vascular Surgery. Vol. 5, St Louis, Missouri: Quality Medical Publishing Inc, 1993:434‐40.
Zogogiannis 2011 {published data only}
-
- Zogogiannis ID, Iatrou CA, Lazarides MK, Vogiatzaki TD, Wachtel MS, Chatzigakis PK, et al. Evaluation of an intraoperative algorithm based on near‐infrared refracted spectroscopy monitoring, in the intraoperative decision for shunt placement, in patients undergoing carotid endarterectomy.. Middle East Journal of Anesthesiology 2011;21:367‐73. - PubMed
Additional references
ACAS 1995
-
- Executive Committee for the Asymptomatic Carotid Atherosclerosis study. Endarterectomy for asymptomatic carotid artery stenosis. JAMA 1995;273:1421‐8. - PubMed
ACST 2004
-
- ACST Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Lancet 2004;363:1491‐502. - PubMed
APT 1994
Benjamin 1993
-
- Benjamin ME, Silva MB, Watt C, McCaffrey MT, Burford‐Foggs A, Flinn WR. Awake patient monitoring to determine the need for shunting during carotid endarterectomy. Surgery 1993;114:673‐81. - PubMed
Bond 2002
-
- Bond R, Warlow C P, Naylor AR, Rothwell PM. Variation in surgical and anaesthetic technique and associations with operative risk in the European Carotid Surgery Trial: implications for trials of ancillary techniques. European Journal of Vascular and Endovascular Surgery 2002;23:117‐26. - PubMed
Buche 1988
-
- Buche M, Grenier Y, Schoevaerdts JC, Jaumin P, Ponlot R, Chalant CH. Comparative results after endarterectomy of internal carotid artery performed with or without a shunt. Journal of Cardiovascular Surgery 1988;29:428‐31. - PubMed
Connolly 1977
ECST 1991
-
- European Carotid Surgery Trialists Collaborative Group. MRC Carotid Surgery Trial: interim results for symptomatic patients with severe (70‐99%) or with mild (0‐29%) carotid stenosis. Lancet 1991;337:1235‐43. - PubMed
Evans 1985
-
- Evans WE, Hayes JP, Waltke, EA, Vermilion BD. Optimal cerebral monitoring during carotid endarterectomy: neurologic response under local anaesthetic. Journal of Vascular Surgery 1985;2:775‐7. - PubMed
Fode 1986
-
- Fode NC, Sundt TM, Robertson JT, Peerless SJ, Shields CB. Multicenter retrospective review of results and complications of carotid endarterectomy in 1981. Stroke 1986;17:370‐5. - PubMed
Forssell 1995
-
- Forssell C, Kitzing P, Bergqvist D. Cranial nerve injuries after carotid surgery. A prospective study of 663 operations. European Journal of Vascular Surgery 1995;10:445‐9. - PubMed
Girn 2008
-
- Girn HR, Dellagrammaticas D, Laughlan K, Gough MJ, for the GALA Trial Collaborators. Carotid endarterectomy: technical practices of surgeons participating in the GALA trial. European Journal of Vascular and Endovascular Surgery 2008;36:385‐9. - PubMed
Goodney 2012
Green 1985
Halsey 1992
-
- Halsey JH Jr. Risks and benefits of shunting in carotid endarterectomy. The International Transcranial Doppler Collaborators. Stroke 1992;23:1583‐7. - PubMed
Hamdan 1999
-
- Hamdan AD, Pomposelli FB Jr, Gibbons GW, Campbell DR, LoGerfo FW. Perioperative strokes after 1001 consecutive carotid endarterectomy procedures without an electroencephalogram: incidence, mechanism, and recovery. Archives of Surgery 1999;134:412‐5. - PubMed
Hertzer 1997
-
- Hertzer NR, O'Hara PJ, Mascha EJ, Krajewski LP, Sullivan TM, Beven EG. Early outcome assessment for 2228 consecutive carotid endarterectomy procedures: the Cleveland Clinic experience from 1989 to 1995. Journal of Vascular Surgery 1997;26:1‐10. - PubMed
Higgins 2003
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Irwig 1994
-
- Irwig L, Tosteson ANA, Gatsonis C, Lau J, Colditz G, Chalmers TC, et al. Guidelines for meta‐analyses evaluating diagnostic tests. Annals of Internal Medicine 1994;120:667‐76. - PubMed
Javid 1979
-
- Javid H, Julian OC, Dye WS, Hunter JA, Najafi H, Goldin MD, et al. Seventeen‐year experience with routine shunting in carotid surgery. World Journal of Surgery 1979;3:167‐77. - PubMed
Lewis 2008
-
- Lewis SC, Warlow CP, Bodenham AR, Colam B, Rothwell PM, Torgerson D, et al. General anaesthesia versus local anaesthesia for carotid surgery (GALA): a multicentre, randomised controlled trial. Lancet 2008;372:2132‐42. - PubMed
NASCET 1991
-
- North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high‐grade carotid stenosis. New England Journal of Medicine 1991;325:445‐765. - PubMed
Nguyen 2005
-
- Nguyen TQ, Lind L, Harris EJ Jr. Selective shunting during carotid endarterectomy. Vascular 2005;13:23‐7. - PubMed
Ott 1980
Ouriel 1987
-
- Ouriel K, Green RM. Clinical and technical factors influencing recurrent carotid stenosis and occlusion after endarterectomy. Journal of Vascular Surgery 1987;5:702‐6. - PubMed
Prioleau 1977
Reddy 1987
-
- Reddy K, West M, Anderson B. Carotid endarterectomy without indwelling shunts and intraoperative electrophysiologic monitoring. Canadian Journal of Neurological Sciences 1987;14:131‐5. - PubMed
Rerkasem 2009
-
- Rerkasem K, Rothwell PM. Temporal trends in the risks of stroke and death due to carotid endarterectomy for symptomatic carotid stenosis: an updated systematic review. European Journal of Vascular and Endovascular Surgery 2009;37:504‐11. - PubMed
Rerkasem 2011
RevMan 2012 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Ricotta 1983
Rothwell 1996
-
- Rothwell PM, Slattery J, Warlow CP. A systematic review of the risk of stroke and death due to endarterectomy for symptomatic carotid stenosis. Stroke 1996;27:260‐5. - PubMed
Salvian 1997
-
- Salvian AJ, Taylor DC, Hsiang YN, Hildebrand HD, Litherland HK, Humer MF, et al. Selective shunting with EEG monitoring is safer than routine shunting for carotid endarterectomy. Cardiovascular Surgery 1997;5:481‐5. - PubMed
Schulz 1995
-
- Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995;273:408‐12. - PubMed
Schweiger 1988
-
- Schweiger H, Kamp H‐D, Dinkel M. Somatosensory evoked potentials (SEP) during carotid endarterectomy ‐ end of shunt debate?. In: Boccalon H editor(s). Angiology: Strategy for Diagnosis and Therapeutics. Paris: John Libbey Eurotext, 1988:353‐5.
Steiger 1989
-
- Steiger HJ, Schaffer L, Boll J, Liechti S. Results of microsurgical carotid endarterectomy. A prospective study with transcranial Doppler and EEG monitoring, and elective shunting. Acta Neurochirurgica 1989;100:31‐8. - PubMed
Sundt 1986
Thompson 1979
-
- Thompson JE. Complications of carotid endarterectomy and their prevention. World Journal of Surgery 1979;3:155‐65. - PubMed
Vaniyapong 2013
Whittemore 1983
Wilkinson 1997
-
- Wilkinson JM, Rochester JR, Sivaguru A, Cameron IC, Fisher R, Beard JD. Middle cerebral artery blood velocity, embolization, and neurological outcome during carotid endarterectomy. European Journal of Vascular and Endovascular Surgery 1997;14:402. - PubMed
Woodworth 2007
-
- Woodworth GF, McGirt MJ, Than KD, Huang J, Perler BA, Tamargo RJ. Selective versus routine intraoperative shunting during carotid endarterectomy: a multivariate outcome analysis. Neurosurgery 2007;61:1170‐6. - PubMed
References to other published versions of this review
Bond 2002a
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources