

Ultrasound and shockwave therapy for acute fractures in adults
- PMID: 24956457
- PMCID: PMC7173732
- DOI: 10.1002/14651858.CD008579.pub3
Ultrasound and shockwave therapy for acute fractures in adults
Update in
-
Ultrasound and shockwave therapy for acute fractures in adults.Cochrane Database Syst Rev. 2023 Mar 3;3(3):CD008579. doi: 10.1002/14651858.CD008579.pub4. Cochrane Database Syst Rev. 2023. PMID: 36866917 Free PMC article.
Abstract
Background: The morbidity and socioeconomic costs of fractures are considerable. The length of time to healing is an important factor in determining a person's recovery after a fracture. Ultrasound may have a therapeutic role in reducing the time to union after fracture. This is an update of a review previously published in February 2012.
Objectives: To assess the effects of low-intensity ultrasound (LIPUS), high-intensity focused ultrasound (HIFUS) and extracorporeal shockwave therapies (ECSW) as part of the treatment of acute fractures in adults.
Search methods: We searched the Cochrane Bone, Joint and Muscle Trauma Group Specialised Register (2 June 2014), the Cochrane Central Register of Controlled Trials (The Cochrane Library 2014, Issue 5), MEDLINE (1946 to May Week 3 2014), EMBASE (1980 to 2014 Week 22), trial registers and reference lists of articles.
Selection criteria: Randomised and quasi-randomised controlled trials evaluating ultrasound treatment in the management of acute fractures in adults. Studies had to include participants over 18 years of age with acute fractures, reporting outcomes such as function; time to union; non-union; secondary procedures such as for fixation or delayed union or non-union; adverse effects; pain; costs; and patient adherence.
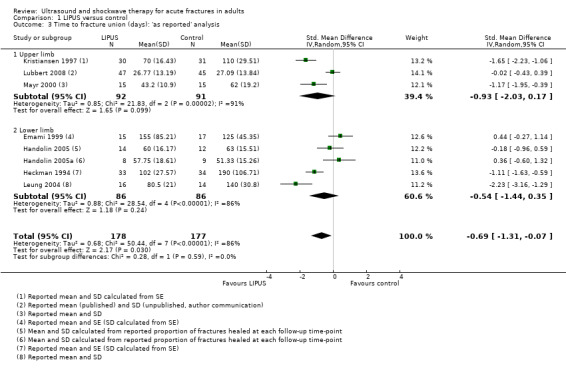
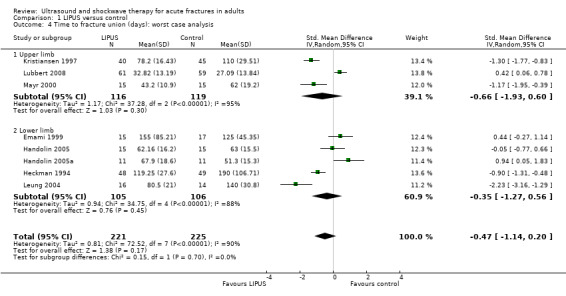
Data collection and analysis: Two authors independently extracted data from the included studies. Treatment effects were assessed using mean differences, standardised mean differences or risk ratios using a fixed-effect model, except where there was substantial heterogeneity, when data were pooled using a random-effects model. Results from 'worst case' analyses, which gave more conservative estimates of treatment effects for time to fracture union, are reported in preference to those from 'as reported' analyses.
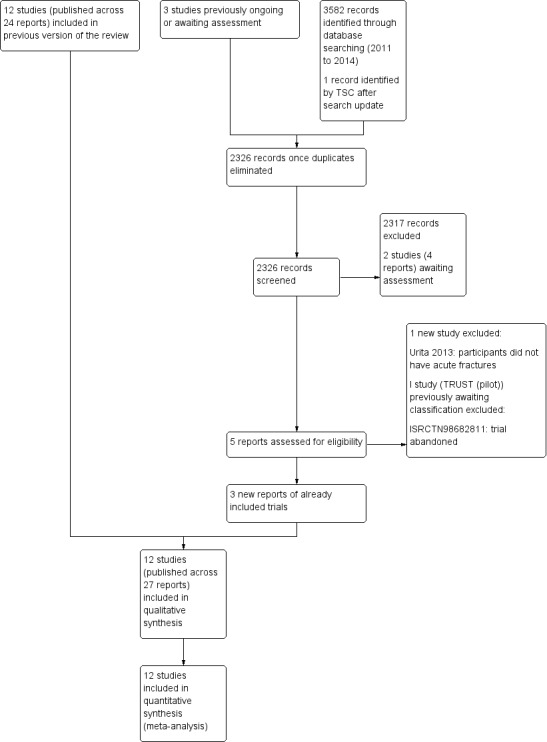
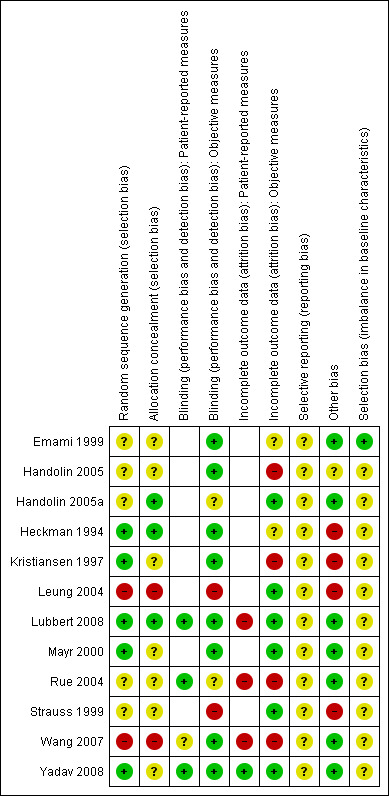
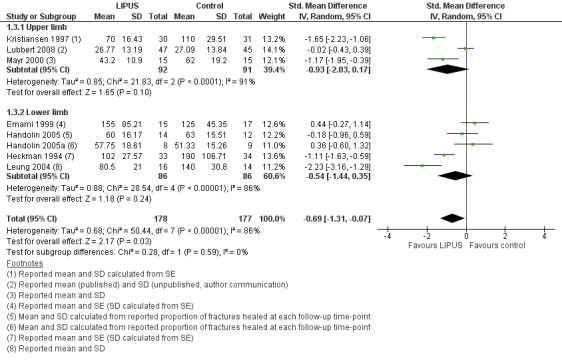
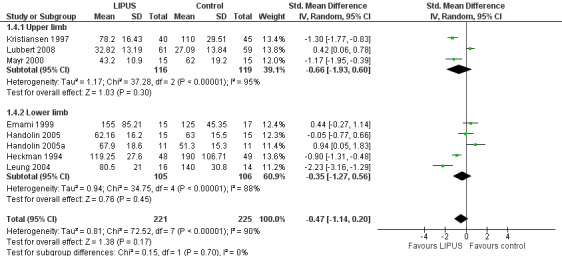
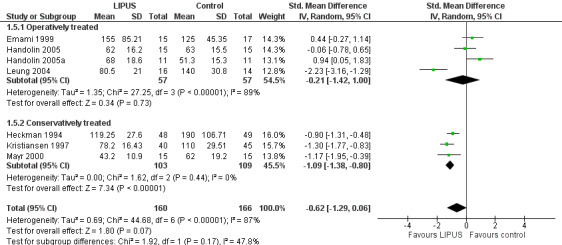
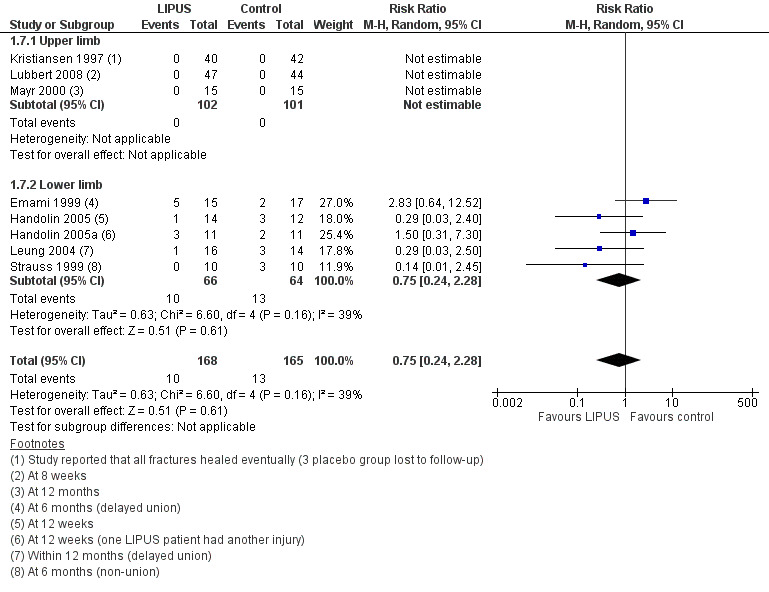
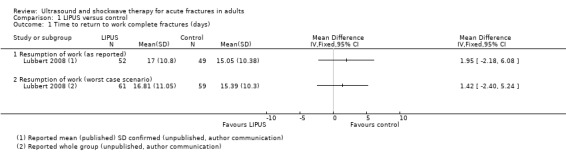
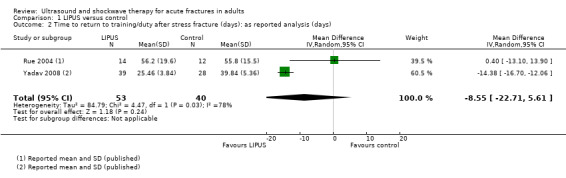
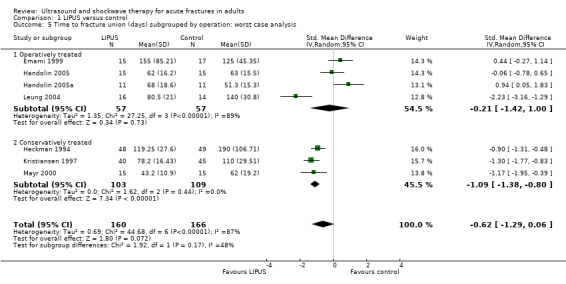
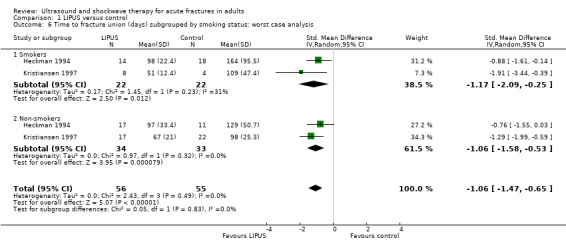
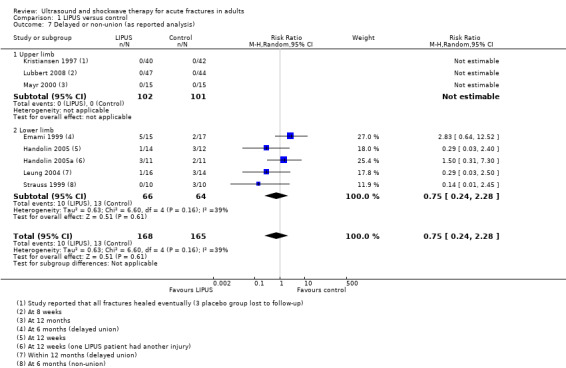
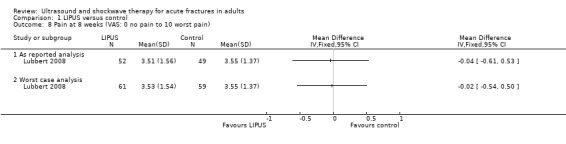
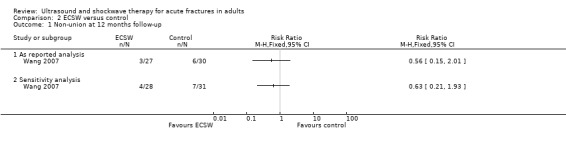
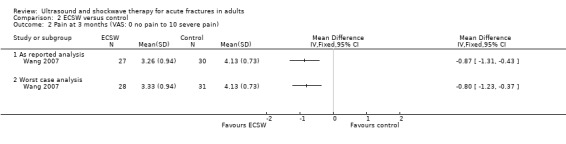
Main results: We included 12 studies, involving 622 participants with 648 fractures. Eight studies were randomised placebo-controlled trials, two were randomised controlled trials without placebo controls, one was a quasi-randomised placebo-controlled trial and one was a quasi-randomised controlled trial without placebo control. Eleven trials tested LIPUS and one trial tested ECSW. Four trials included participants with conservatively treated upper limb complete fractures and six trials included participants with lower limb complete fractures; these were surgically fixed in four trials. The remaining two trials reported results for conservatively treated tibial stress fractures.'Risk of bias' assessment of the included studies was hampered by the poor reporting of methods, frequently resulting in the risk of bias of individual domains being judged as 'unclear'. Both quasi-randomised studies were at high risk of bias, including selection and attrition bias. Three studies were at low risk of selection bias relating to allocation concealment the majority of studies were at low risk of performance bias as they employed a form of intervention blinding.Only limited data were available from three of only four studies reporting on functional outcome. One study of complete fractures found little evidence of a difference between the two groups in the time to return to work (mean difference (MD) 1.95 days favouring control, 95% confidence interval (CI) -2.18 to 6.08; 101 participants). Pooled data from two studies found LIPUS did not significantly affect the time to return to training or duty in soldiers or midshipmen with stress fractures (MD -8.55 days, 95% CI -22.71 to 5.61; 93 participants).We adopted a conservative strategy for data analysis that was more likely to underestimate than to overestimate a benefit of the intervention. After pooling results from eight studies (446 fractures), the data showed no statistically significant reduction in time to union of complete fractures treated with LIPUS (standardised mean difference (SMD) -0.47, 95% CI -1.14 to 0.20). This result could include a clinically important benefit or harm, and should be seen in the context of the highly significant statistical heterogeneity (I² = 90%). This heterogeneity was not explained by the a priori subgroup analyses (upper limb versus lower limb fracture, smoking status). An additional subgroup analysis comparing conservatively and operatively treated fractures raised the possibility that LIPUS may be effective in reducing healing time in conservatively managed fractures, but the test for subgroup differences did not confirm a significant difference between the subgroups.Pooled results from five of the eight trials (333 fractures) reporting proportion of delayed union or non-union showed no significant difference between LIPUS and control (10/168 versus 13/165; RR 0.75; 95% CI 0.24 to 2.28). Adverse effects directly associated with LIPUS and associated devices were found to be few and minor, and compliance with treatment was generally good. One study reporting on pain scores found no difference between groups at eight weeks (101 participants).One quasi-randomised study found no significant difference in non-union at 12 months between internal fixation supplemented with ECSW and internal fixation alone (3/27 versus 6/30; RR 0.56, 95% CI 0.15 to 2.01). There was a clinically small but statistically significant difference in the visual analogue scores for pain in favour of ECSW at three month follow-up (MD -0.80, 95% CI -1.23 to -0.37). The only reported complication was infection, with no significant difference between the two groups.
Authors' conclusions: While a potential benefit of ultrasound for the treatment of acute fractures in adults cannot be ruled out, the currently available evidence from a set of clinically heterogeneous trials is insufficient to support the routine use of this intervention in clinical practice. Future trials should record functional outcomes and follow-up all trial participants.
Conflict of interest statement
XL Griffin: XG, nor his institution, have received any grants pertaining to this published work. XG has been in receipt of several institutional grants to support other academic interests. ML Costa: MC, nor his institution, have received any grants pertaining to this published work. MC has been in receipt of several institutional grants to support other academic interests. N Parsons: none known D Metcalfe: none known
Figures
Update of
-
Ultrasound and shockwave therapy for acute fractures in adults.Cochrane Database Syst Rev. 2012 Feb 15;(2):CD008579. doi: 10.1002/14651858.CD008579.pub2. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2014 Jun 23;(6):CD008579. doi: 10.1002/14651858.CD008579.pub3. PMID: 22336847 Updated.
References
References to studies included in this review
Emami 1999 {published data only}
-
- Emami A, Petren‐Mallmin M, Larsson S. No effect of low‐intensity ultrasound on healing time of intramedullary fixed tibial fractures. Journal of Orthopaedic Trauma 1999;13(4):252‐7. - PubMed
Handolin 2005 {published data only (unpublished sought but not used)}
-
- Handolin L, Kiljunen V, Arnala I, Kiuru MJ, Pajarinen J, Partio EK, et al. No long‐term effects of ultrasound therapy on bioabsorbable screw‐fixed lateral malleolar fracture. Scandinavian Journal of Surgery 2005;94(3):239‐42. - PubMed
-
- Handolin L, Kiljunen V, Arnala I, Pajarinen J, Partio EK, Rokkanen P. The effect of low intensity ultrasound and bioabsorbable self‐reinforced poly‐L‐lactide screw fixation on bone in lateral malleolar fractures. Archives of Orthopaedic and Trauma Surgery 2005;125(5):317‐21. - PubMed
Handolin 2005a {published data only (unpublished sought but not used)}
-
- Handolin L, Kiljunen V, Arnala I, Kiuru M, Pajarinen J, Partio E, et al. The effects of low‐intensity ultrasound on 22 bioabrorbable self‐reinforced poly‐L‐lactic acid (SR‐PLLA) screw fixed lateral malleolar fracture. Suomen Ortopedia ja Traumatologia 2004; Vol. 27, issue 4:236‐8.
-
- Handolin L, Kiljunen V, Arnala I, Kiuru MJ, Pajarinen J, Partio EK, et al. Effect of ultrasound therapy on bone healing of lateral malleolar fractures of the ankle joint fixed with bioabsorbable screws. Journal of Orthopaedic Science 2005;10(4):391‐5. - PubMed
Heckman 1994 {published and unpublished data}
-
- Cook S, Ryaby JP, Heckmann JD, Kristiansen TK. Low‐intensity pulsed ultrasound accelerates tibia and distal radius fracture healing in smokers. Hefte zur der Unfallchirurg 1996;262:336.
-
- Cook SD, Ryaby JP, McCabe J, Frey JJ, Heckman JD, Kristiansen TK. Acceleration of tibia and distal radius fracture healing in patients who smoke. Clinical Orthopaedics & Related Research 1997;(337):198‐207. - PubMed
-
- Cook SD, Ryaby JP, McCabe J, Frey JJ, Heckman JD, Kristiansen TK. Low intensity pulsed ultrasound accelerates tibia and distal radius fracture healing in smokers [abstract]. Orthopaedic Transactions 1996;20(1):56.
-
- Heckman JD. Personal communication September 2 2010.
-
- Heckman JD, Ryaby JP, McCabe J, Frey JJ, Kilcoyne RF. Acceleration of tibial fracture‐healing by non‐invasive, low‐intensity pulsed ultrasound. Journal of Bone and Joint Surgery ‐ American Volume 1994;76(1):26‐34. - PubMed
Kristiansen 1997 {published and unpublished data}
-
- Cook S, Ryaby JP, Heckmann HD, Kristiansen TK. Low‐intensity pulsed ultrasound accelerates tibia and distal radius fracture healing in smokers. Hefte zur der Unfallchirurg 1996;262:336.
-
- Cook SD, Ryaby JP, McCabe J, Frey JJ, Heckman JD, Kristiansen TK. Acceleration of tibia and distal radius fracture healing in patients who smoke. Clinical Orthopaedics and Related Research 1997;337:198‐207. - PubMed
-
- Cook SD, Ryaby JP, McCabe J, Frey JJ, Heckman JD, Kristiansen TK. Low intensity pulsed ultrasound accelerates tibia and distal radius fracture healing in smokers [abstract]. Orthopaedic Transactions 1996;20(1):56.
-
- Kristiansen TK. The effect of low power specifically programmed ultrasound on the healing time of fresh fractures using a Colles model [abstract]. Journal of Orthopaedic Trauma 1990;4(2):227.
-
- Kristiansen TK, Ryaby JP, McCabe J, Frey J. Controlling loss of reduction in distal radius fractures in an randomized, double‐blind study using low‐intensity ultrasound. Hefte zur der Unfallchirurg. 1996; Vol. 262:369.
Leung 2004 {published data only}
-
- Leung KS, Lee WS, Tsui HF, Liu PPL, Cheung WH. Complex tibial fracture outcomes following treatment with low‐intensity pulsed ultrasound. Ultrasound in Medicine and Biology 2004;30(3):389‐95. - PubMed
Lubbert 2008 {published and unpublished data}
-
- Lubbert PH. Personal communication November 7 2010.
-
- Lubbert PHW, Rijt RHH, Hoorntje LE, Werken C. Low‐intensity pulsed ultrasound (LIPUS) in fresh clavicle fractures: A multi‐centre double blind randomised controlled trial. Injury 2008;39(12):1444‐52. - PubMed
Mayr 2000 {published data only}
-
- Mayr E. Accelerated healing of scaphoid fracture ‐ a randomized study [abstract]. Journal of Bone and Joint Surgery ‐ British Volume 1999;81 Suppl 2:206.
-
- Mayr E, Rudzki M, Borchardt B, Ruter A. Accelerated healing of scaphoid fractures ‐ A randomized study [abstract]. Journal of Orthopaedic Trauma 1999;13(4):310.
-
- Mayr E, Rudzki M‐M, Rudzki M, Borchardt B, Hausser H, Ruter A. Does pulsed low‐Intensity ultrasound accelerate healing of scaphoid fractures? [Beschleunigt niedrig intensive, gepulster Ultraschall die Heilung von Skaphoidfrakturen?]. Handchirurgie Mikrochirurgie Plastische Chirurgie 2000;32(2):115‐22. - PubMed
Rue 2004 {published data only}
-
- Rue JP, Armstrong DW 3rd, Frassica FJ, Deafenbaugh M, Wilckens JH. The effect of pulsed ultrasound in the treatment of tibial stress fractures. Orthopedics 2004;27(11):1192‐5. - PubMed
Strauss 1999 {published data only (unpublished sought but not used)}
-
- Strauss E, McCabe J. Treatment of Jones fractures of the foot with adjunctive use of pulsed low‐intensity ultrasound stimulation [abstract]. American Academy of Orthopaedic Surgeons Annual Meeting; 1998 Mar 13‐14; New Orleans. 1998.
-
- Strauss E, Ryaby JP, McCabe J. Treatment of Jones' fractures of the foot with adjunctive use of low‐pulsed ultrasound stimulation. Journal of Orthopaedic Trauma 1999;13(4):310.
Wang 2007 {published data only}
-
- Liu HC, Fu TH. Effects of shockwave on acute high‐energy fractures of the femur and tibia [abstract]. American Academy of Orthopaedic Surgeons Annual Meeting; 2007 Feb 14–18; San Diego. 2007.
-
- Wang CJ, Liu HC, Fu TH. The effects of extracorporeal shockwave on acute high‐energy long bone fractures of the lower extremity. Archives of Orthopaedic and Trauma Surgery 2007;127(2):137‐42. - PubMed
References to studies excluded from this review
Basso 1998 {published data only}
-
- Basso O, Pike JM. The effect of low frequency, long‐wave ultrasound therapy on joint mobility and rehabilitation after wrist fracture. Journal of Hand Surgery ‐ British Volume 1998;23(1):136‐9. - PubMed
Busse 2005 {published data only}
-
- Busse JW, Bhandari M, Sprague S, Johnson‐Masotti AP, Gafni A. An economic analysis of management strategies for closed and open grade I tibial shaft fractures. Acta Orthopaedica 2005;76(5):705‐12. - PubMed
Heckman 1997 {published data only}
-
- Heckman JD, Sarasohn‐Kahn J. The economics of treating tibia fractures: The cost of delayed unions. Bulletin of The Hospital for Joint Dieases 1997;56(1):63‐72. - PubMed
ISRCTN98682811 {unpublished data only}
-
- Bhandari M, Busse J, Guyatt G. Trial to re‐evaluate ultrasound in the treatment of tibial fractures (TRUST). http://www.controlled‐trials.com/ISRCTN98682811 (accessed 14 June 2011). - PMC - PubMed
-
- Busse J. Personal communication 15 October 2013.
Urita 2013 {published data only}
-
- Urita A, Iwasaki N, Kondo M, Nishio Y, Kamishima T, Minami A. Effect of low‐intensity pulsed ultrasound on bone healing at osteotomy sites after forearm bone shortening. Journal of Hand Surgery (American) 2013;38(3):498‐503. - PubMed
References to studies awaiting assessment
ISRCTN90844675 {unpublished data only}
-
- Seifert J. Personal communication. 30 October 2013.
-
- Seifert J. Pulsed ultrasound to speed‐up healing after intramedullary nailing of tibia fractures (PUSH‐IT). http://controlled‐trials.com/ISRCTN90844675/ISRCTN90844675 (accessed 9 December 2011).
NCT00667849 {published and unpublished data}
-
- Bhandari M. Trial to re‐evaluate ultrasound in the treatment of tibial fractures (TRUST). http://www.clinicaltrials.gov/ct2/show/NCT00667849 (accessed 7 December 2011). - PMC - PubMed
-
- Busse J. Personal communication 15 October 2013.
Additional references
Aaron 2004
-
- Aaron RK, Ciombor DM, Simon BJ. Treatment of nonunions with electric and electromagnetic fields. Clinical Orthopaedics & Related Research 2004;(419):21‐9. [PUBMED: 15021127] - PubMed
Boutron 2008
-
- Boutron I, Moher D, Altman DG, Schulz KF, Ravaud P, CONSORT Group. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: explanation and elaboration. Annals of Internal Medicine 2008;148(4):295‐309. - PubMed
Busse 2009
Busse 2013
-
- Busse J. Personal communication 15 October 2013.
Busse 2014
Cook 1997
-
- Cook SD, Ryaby JP, McCabe J, Frey JJ, Heckman JD, Kristiansen TK. Acceleration of tibia and distal radius fracture healing in patients who smoke. Clinical Orthopaedics & Related Research 1997;(337):198‐207. - PubMed
Dijkman 2011
Einhorn 1995
-
- Einhorn TA. Enhancement of fracture healing. Journal of Bone & Joint Surgery ‐ American Volume 1995;77(6):940‐56. [MEDLINE: ] - PubMed
Griffin 2008
-
- Griffin XL, Costello I, Costa ML. The role of low intensity pulsed ultrasound therapy in the management of acute fractures: a systematic review. Journal of Trauma‐Injury Infection & Critical Care 2008;65(6):1446‐52. [PUBMED: 19077640] - PubMed
Hadjiargyrou 1998
-
- Hadjiargyrou M, McLeod K, Ryaby JP, Rubin C. Enhancement of fracture healing by low intensity ultrasound. Clinical Orthopaedics & Related Research 1998;(355 Suppl):S216‐29. [PUBMED: 9917641] - PubMed
Handolin 2005b
-
- Handolin L, Kiljunen V, Arnala I, Kiuru MJ, Pajarinen J, Partio EK, et al. No long‐term effects of ultrasound therapy on bioabsorbable screw‐fixed lateral malleolar fracture. Scandinavian Journal of Surgery 2005;94(3):239‐42. - PubMed
Higgins 2003
Higgins 2008
-
- Higgins JPT, Altman DG. Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Chichester: John Wiley & Sons, 2008.
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Reher 1997
-
- Reher P, Elbeshir el‐NI, Harvey W, Meghji S, Harris M. The stimulation of bone formation in vitro by therapeutic ultrasound. Ultrasound in Medicine & Biology 1997;23(8):1251‐8. [PUBMED: 9372573] - PubMed
Seifert 2013
-
- Seifert J. Personal communication. 30 October 2013.
Victoria 2009
Wang 1994
-
- Wang SJ, Lewallen DG, Bolander ME, Chao EY, Ilstrup DM, Greenleaf JF. Low intensity ultrasound treatment increases strength in a rat femoral fracture model. Journal of Orthopaedic Research 1994;12(1):40‐7. [PUBMED: 8113941] - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical