

Human papillomavirus and overall survival after progression of oropharyngeal squamous cell carcinoma
- PMID: 24958820
- PMCID: PMC4195851
- DOI: 10.1200/JCO.2014.55.1937
Human papillomavirus and overall survival after progression of oropharyngeal squamous cell carcinoma
Abstract
Purpose: Risk of cancer progression is reduced for patients with human papillomavirus (HPV) -positive oropharynx cancer (OPC) relative to HPV-negative OPC, but it is unknown whether risk of death after progression is similarly reduced.
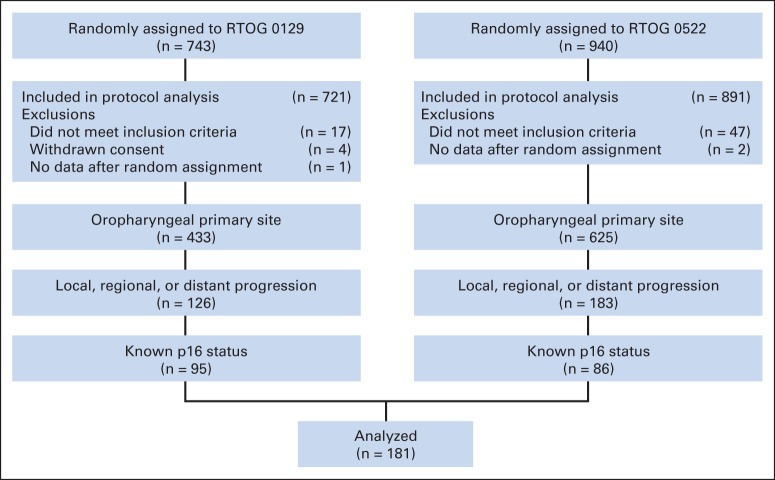
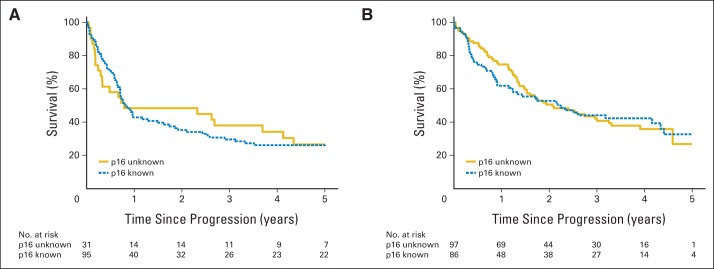
Patients and methods: Patients with stage III-IV OPC enrolled onto Radiation Therapy Oncology Group trials 0129 or RTOG 0522 who had known tumor p16 status plus local, regional, and/or distant progression after receiving platinum-based chemoradiotherapy were eligible for a retrospective analysis of the association between tumor p16 status and overall survival (OS) after disease progression. Rates were estimated by Kaplan-Meier method and compared by log-rank; hazard ratios (HRs) were estimated by Cox models. Tests and models were stratified by treatment protocol.
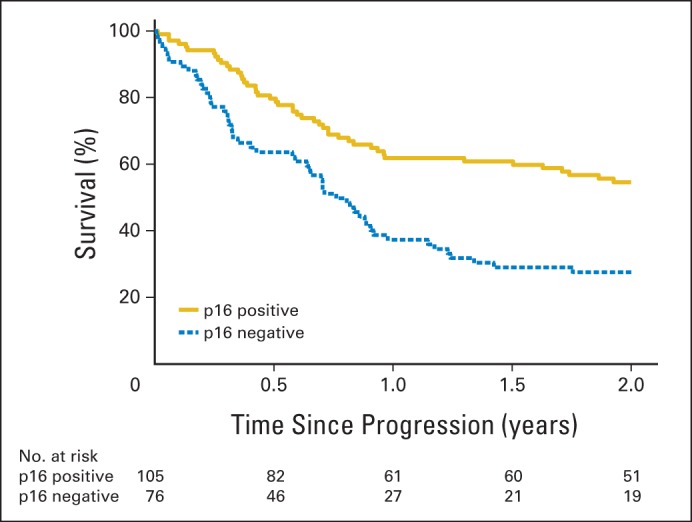
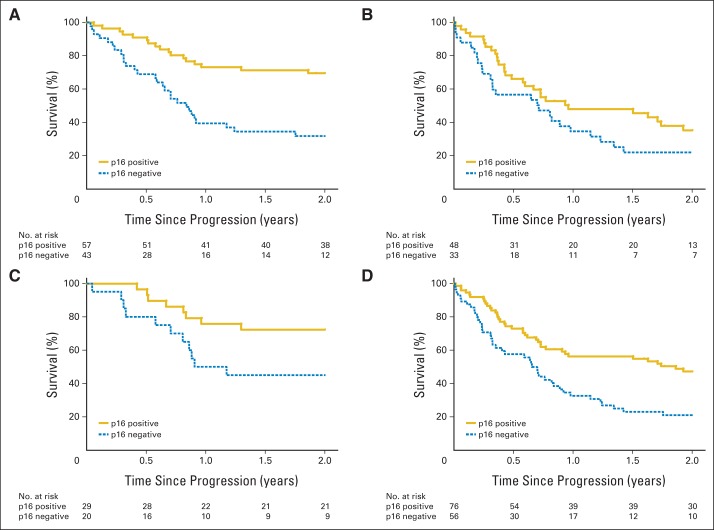
Results: A total of 181 patients with p16-positive (n = 105) or p16-negative (n = 76) OPC were included in the analysis. Patterns of failure and median time to progression (8.2 v 7.3 months; P = .67) were similar for patients with p16-positive and p16-negative tumors. After a median follow-up period of 4.0 years after disease progression, patients with p16-positive OPC had significantly improved survival rates compared with p16-negative patients (2-year OS, 54.6% v 27.6%; median, 2.6 v 0.8 years; P < .001). p16-positive tumor status (HR, 0.48; 95% CI, 0.31 to 0.74) and receipt of salvage surgery (HR, 0.48; 95% CI; 0.27 to 0.84) reduced risk of death after disease progression whereas distant versus locoregional progression (HR, 1.99; 95% CI, 1.28 to 3.09) increased risk, after adjustment for tumor stage and cigarette pack-years at enrollment.
Conclusion: Tumor HPV status is a strong and independent predictor of OS after disease progression and should be a stratification factor for clinical trials for patients with recurrent or metastatic OPC.
© 2014 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
New chapter in our understanding of human papillomavirus-related head and neck cancer.J Clin Oncol. 2014 Oct 20;32(30):3349-52. doi: 10.1200/JCO.2014.56.5754. Epub 2014 Sep 15. J Clin Oncol. 2014. PMID: 25225434 No abstract available.
-
Reply to B. O'Sullivan et Al.J Clin Oncol. 2015 May 20;33(15):1708-9. doi: 10.1200/JCO.2014.60.3555. Epub 2015 Mar 30. J Clin Oncol. 2015. PMID: 25823732 No abstract available.
-
Reply to B. O'Sullivan et Al.J Clin Oncol. 2015 May 20;33(15):1710. doi: 10.1200/JCO.2014.60.3563. Epub 2015 Mar 30. J Clin Oncol. 2015. PMID: 25823736 No abstract available.
-
First Site of Failure Analysis Incompletely Addresses Issues of Late and Unexpected Metastases in p16-Positive Oropharyngeal Cancer.J Clin Oncol. 2015 May 20;33(15):1707-8. doi: 10.1200/JCO.2014.58.2700. Epub 2015 Mar 30. J Clin Oncol. 2015. PMID: 25823739 No abstract available.
References
-
- Fakhry C, Westra WH, Li S, et al. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst. 2008;100:261–269. - PubMed
-
- Huang SH, Perez-Ordonez B, Weinreb I, et al. Natural course of distant metastases following radiotherapy or chemoradiotherapy in HPV-related oropharyngeal cancer. Oral Oncol. 2013;49:79–85. - PubMed
-
- Weinberger PM, Yu Z, Haffty BG, et al. Molecular classification identifies a subset of human papillomavirus–associated oropharyngeal cancers with favorable prognosis. J Clin Oncol. 2006;24:736–747. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
