

Malignant phosphaturic mesenchymal tumor of the pelvis: A report of two cases
- PMID: 24959220
- PMCID: PMC4063565
- DOI: 10.3892/ol.2014.2081
Malignant phosphaturic mesenchymal tumor of the pelvis: A report of two cases
Abstract
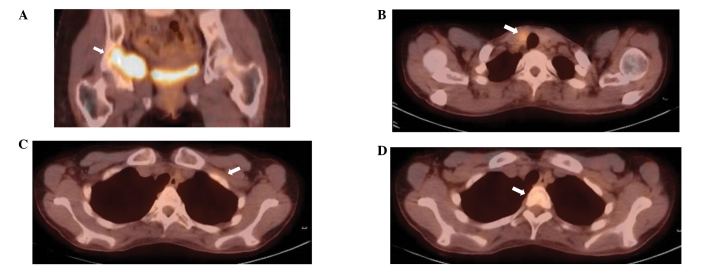
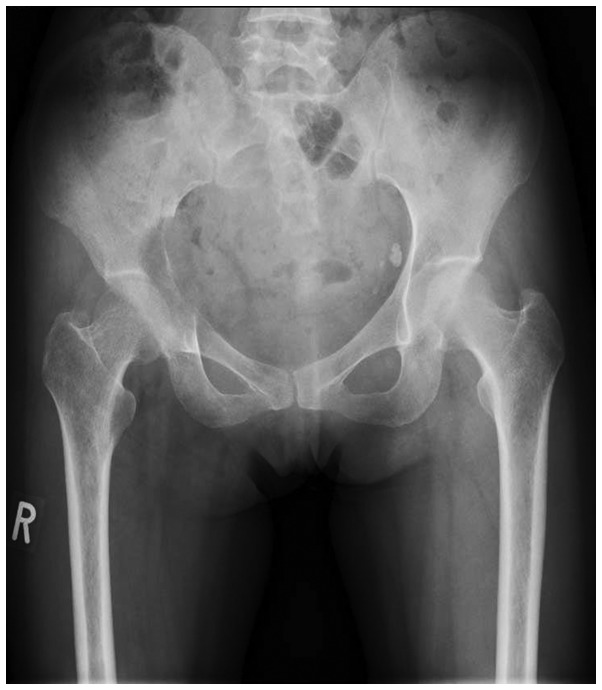
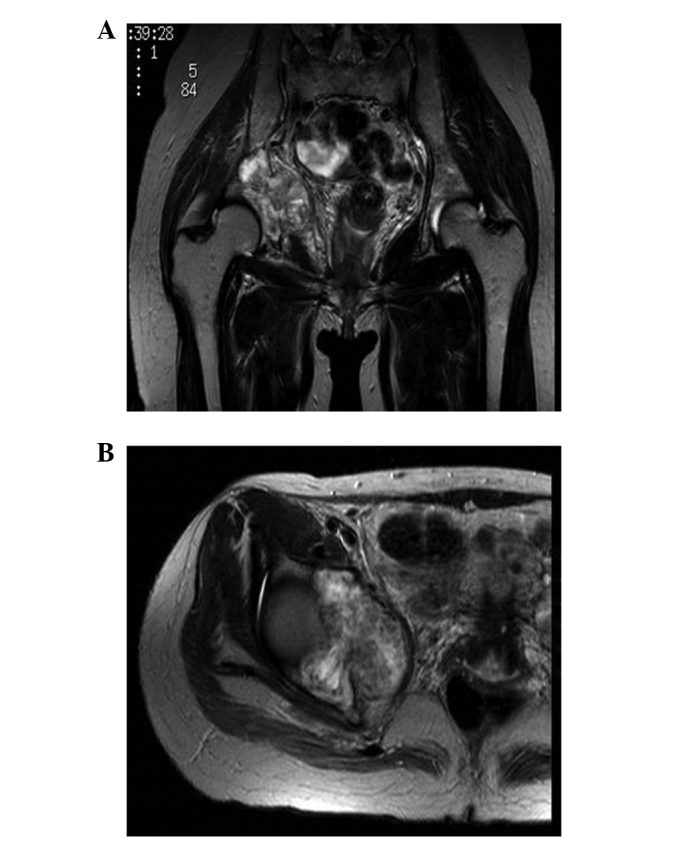
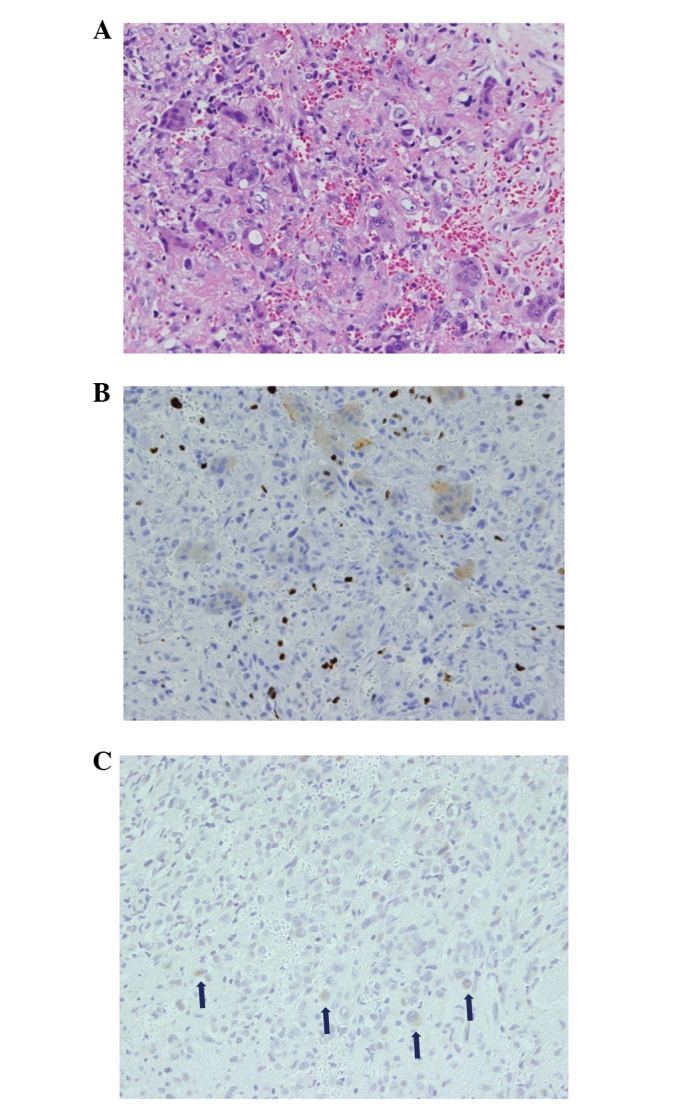
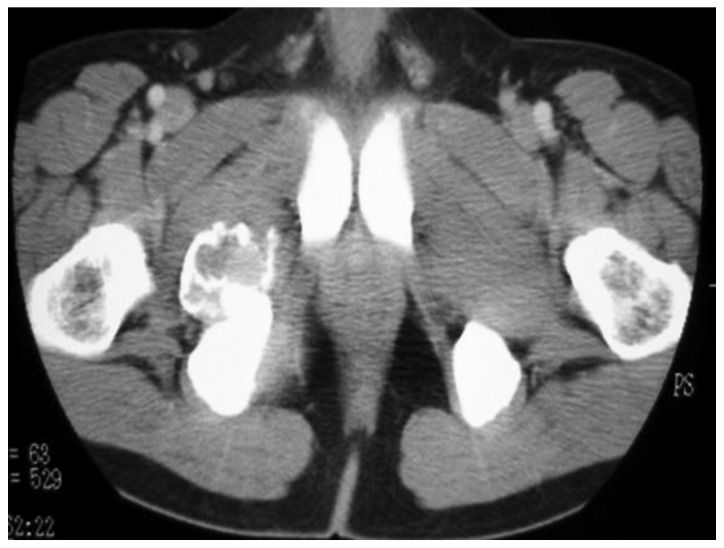
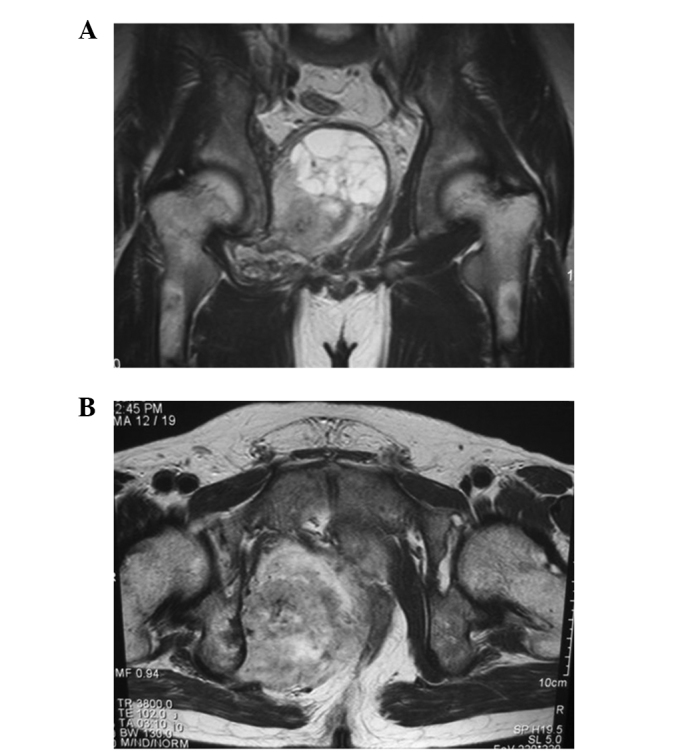
Tumor-induced osteomalacia (TIO) is a rare acquired form of hypophosphatemia commonly associated with phosphaturic mesenchymal tumors (PMTs) located in the bone or soft tissue. Resection of the tumor can cure osteomalacia. Fibroblast growth factor 23 has been identified as a major pathophysiological factor responsible for phosphaturia. The majority of PMTs are benign, and malignant PMTs are uncommon. Even in rare cases, the malignant transformation of PMTs is extremely uncommon. The current study presents two cases in which the patients succumbed to malignant PMTs that developed in the pelvis. The first patient was a 35-year-old female with a malignant PMT occurring as a synchronous double cancer associated with papillary thyroid carcinoma. Diagnosis was difficult, as the multiple uptake on positron emission tomography with 18F-fluorodeoxyglucose presented as pseudofractures mimicking the metastases of thyroid carcinoma. The patient succumbed to rapidly progressive lung metastases. The second patient presented with a pelvic tumor that had developed over 26 years. The patient was diagnosed with a benign PMT by open biopsy and a complete resection was performed. However, two years later, the tumor recurred and lung metastases were observed. The patient ultimately succumbed to respiratory failure due to relapsing lung metastases and disseminated intravascular coagulation. These two cases demonstrate the potential lethality of malignant PMTs and the malignant transformation of benign PMTs. Therefore, TIO patients must be followed up even if diagnosed with a benign tumor. Although TIO is an extremely rare disease, the possibility of malignant PMTs must be recognized.
Keywords: fibroblast growth factor 23; malignant; osteomalacia; phosphaturic mesenchymal tumor; transformation.
Figures

References
-
- Folpe AL, Fanburg-Smith JC, Billings SD, Bisceglia M, Bertoni F, Cho JY, Econs MJ, Inwards CY, Jan de Beur SM, Mentzel T, et al. Most osteomalacia-associated mesenchymal tumors are a single histopathologic entity: an analysis of 32 cases and a comprehensive review of the literature. Am J Surg Pathol. 2004;28:1–30. - PubMed
-
- McCance RA. Osteomalacia with Looser’s nodes (Milkman’s syndrome) due to a raised resistance to vitamin D acquired about the age of 15 years. Q J Med. 1947;16:33–46. - PubMed
-
- Weidner N. Review and update: oncogenic osteomalacia-rickets. Ultrastruct Pathol. 1991;15:317–333. - PubMed
-
- Econs MJ, Drezner MK. Tumor-induced osteomalacia - unveiling a new hormone. N Engl J Med. 1994;330:1679–1681. - PubMed
-
- Ramon I, Kleynen P, Body JJ, Karmali R. Fibroblast growth factor 23 and its role in phosphate homeostasis. Eur J Endocrinol. 2010;162:1–10. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources