

Assessing binocular interaction in amblyopia and its clinical feasibility
- PMID: 24959842
- PMCID: PMC4069064
- DOI: 10.1371/journal.pone.0100156
Assessing binocular interaction in amblyopia and its clinical feasibility
Abstract
Purpose: To measure binocular interaction in amblyopes using a rapid and patient-friendly computer-based method, and to test the feasibility of the assessment in the clinic.
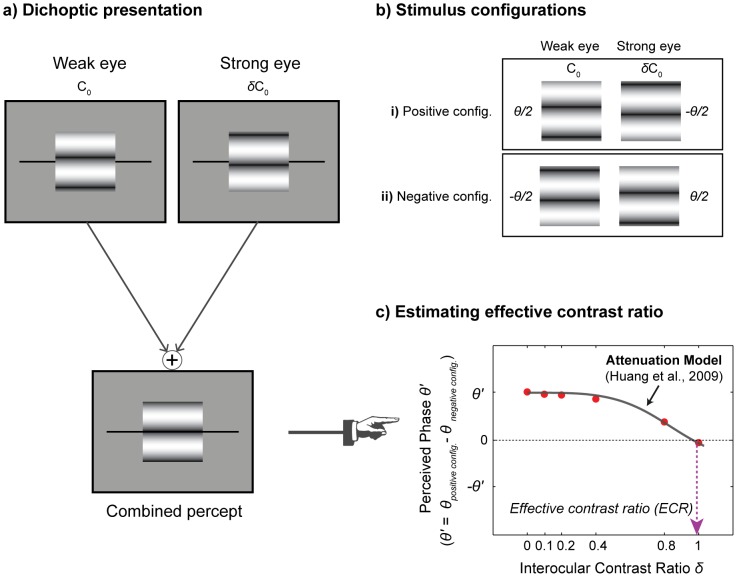
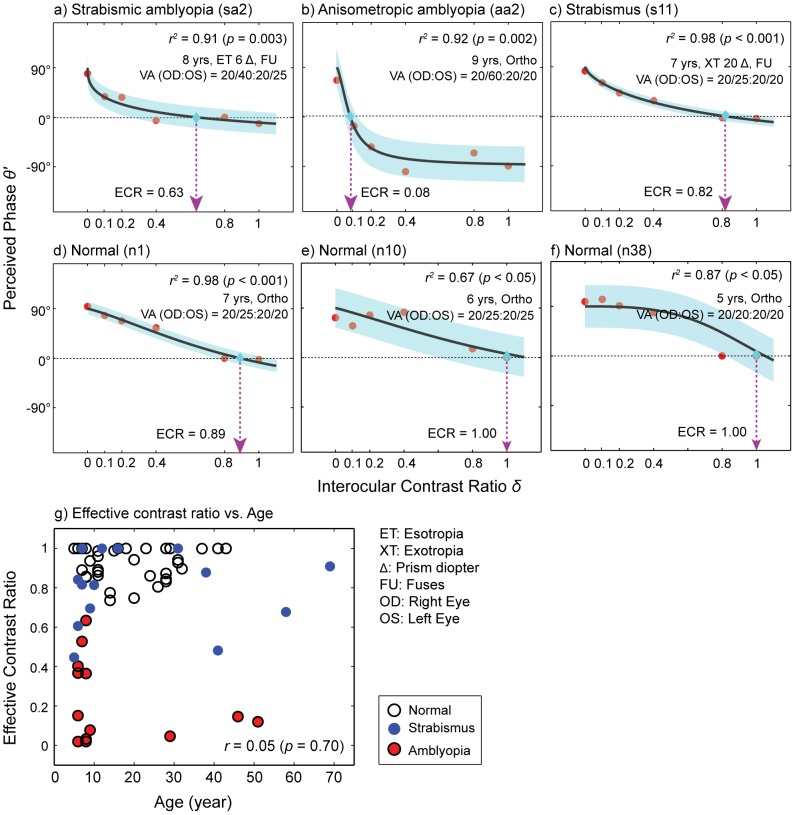
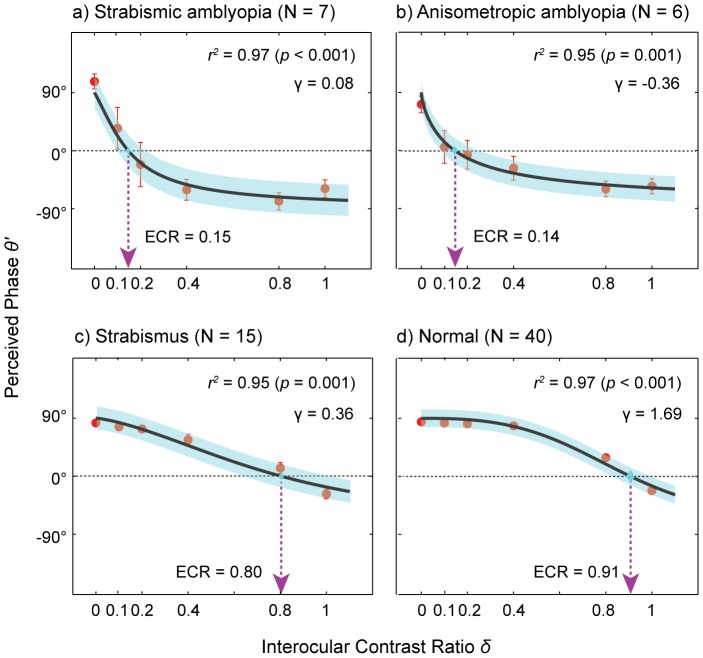
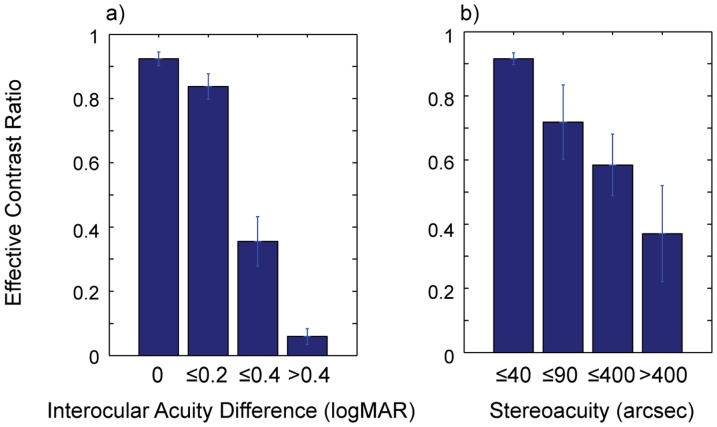
Methods: Binocular interaction was assessed in subjects with strabismic amblyopia (n = 7), anisometropic amblyopia (n = 6), strabismus without amblyopia (n = 15) and normal vision (n = 40). Binocular interaction was measured with a dichoptic phase matching task in which subjects matched the position of a binocular probe to the cyclopean perceived phase of a dichoptic pair of gratings whose contrast ratios were systematically varied. The resulting effective contrast ratio of the weak eye was taken as an indicator of interocular imbalance. Testing was performed in an ophthalmology clinic under 8 mins. We examined the relationships between our binocular interaction measure and standard clinical measures indicating abnormal binocularity such as interocular acuity difference and stereoacuity. The test-retest reliability of the testing method was also evaluated.
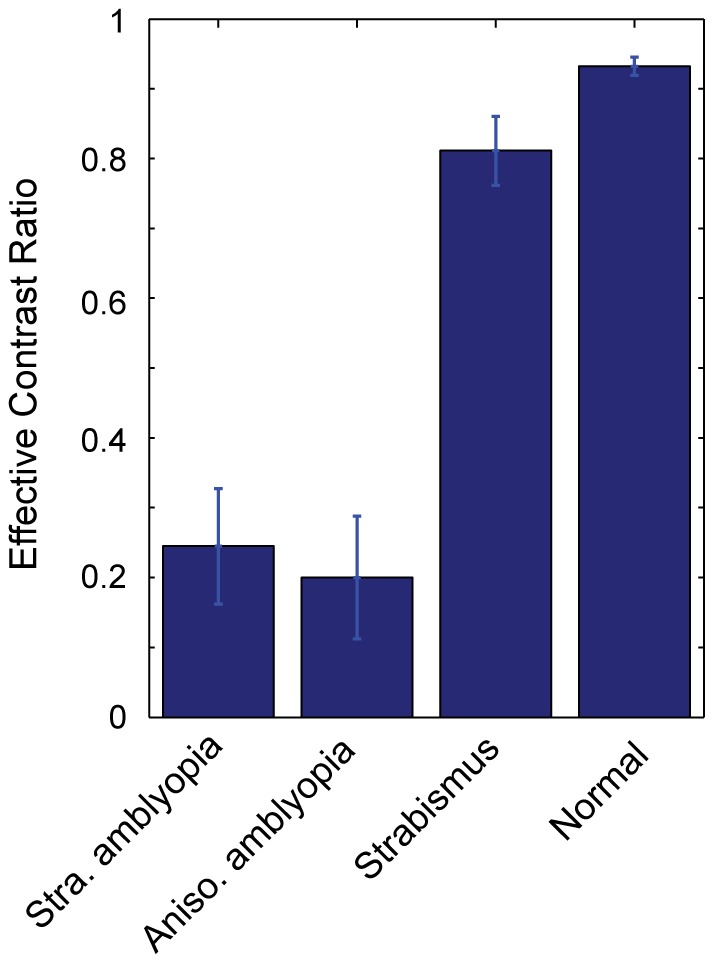
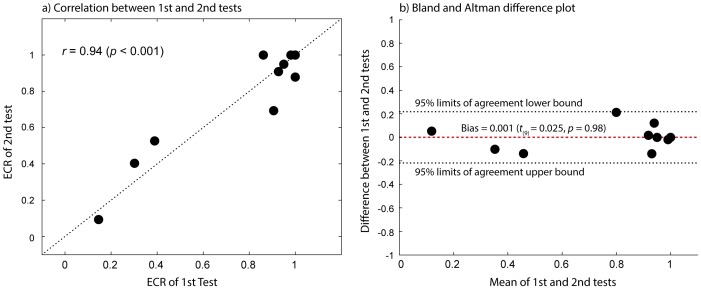
Results: Compared to normally-sighted controls, amblyopes exhibited significantly reduced effective contrast (∼20%) of the weak eye, suggesting a higher contrast requirement for the amblyopic eye compared to the fellow eye. We found that the effective contrast ratio of the weak eye covaried with standard clincal measures of binocular vision. Our results showed that there was a high correlation between the 1st and 2nd measurements (r = 0.94, p<0.001) but without any significant bias between the two.
Conclusions: Our findings demonstrate that abnormal binocular interaction can be reliably captured by measuring the effective contrast ratio of the weak eye and quantitative assessment of binocular interaction is a quick and simple test that can be performed in the clinic. We believe that reliable and timely assessment of deficits in a binocular interaction may improve detection and treatment of amblyopia.
Conflict of interest statement
Figures
References
-
- Hess RF, Campbell FW, Greenhalgh T (1978) On the nature of the neural abnormality in human amblyopia; Neural aberrations and neural sensitivity loss. Pflugers Arch 377: 201–207. - PubMed
-
- Simmons DR (2005) The binocular combination of chromatic contrast. Perception 34: 1035–1042. - PubMed
-
- Levi DM, Klein SA (1985) Vernier acuity, crowding and amblyopia. Vision Res 25: 979–991. - PubMed
-
- Hess RF, Howell ER (1977) The threshold contrast sensitivity function in strabismic amblyopia: Evidence for a two type classification. Vision Res 17: 1049–1055. - PubMed
-
- Hess RF, Mcllhagga W, Field D (1997) Contour integration in strabismic amblyopia: the sufficiency of explanation based on positional uncertainty. Vision Res 37: 3145–3161. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
