

Population-based analysis of invasive fungal infections, France, 2001-2010
- PMID: 24960557
- PMCID: PMC4073874
- DOI: 10.3201/eid2007.140087
Population-based analysis of invasive fungal infections, France, 2001-2010
Abstract
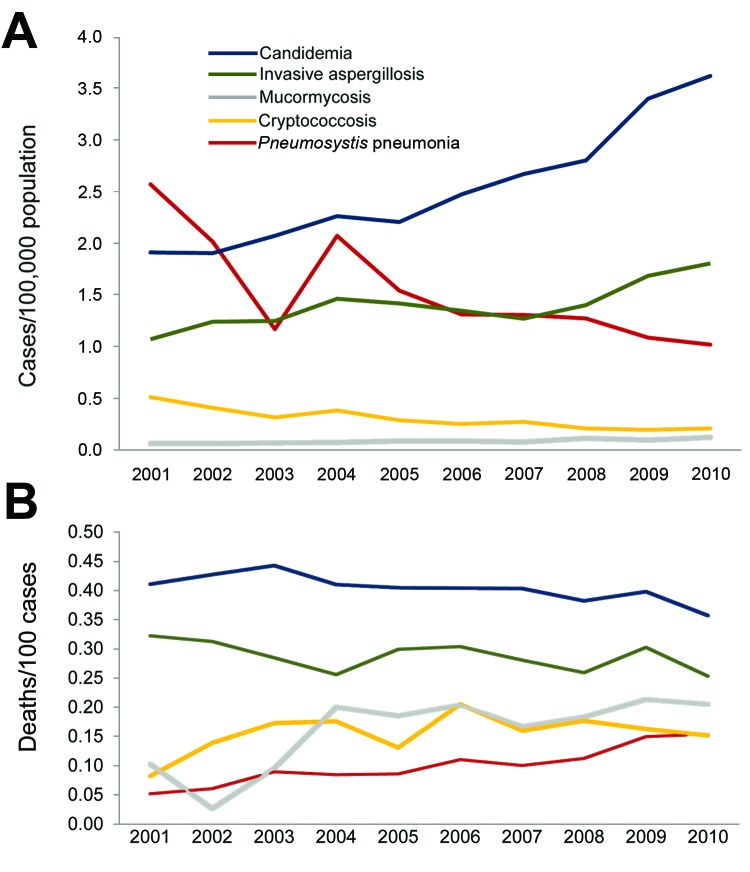
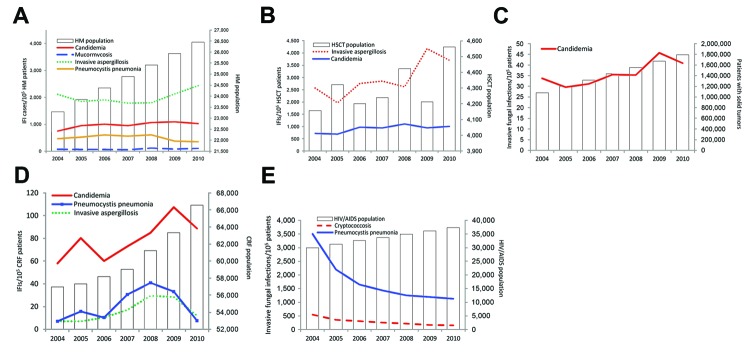
To determine the epidemiology and trends of invasive fungal infections (IFIs) in France, we analyzed incidence, risk factors, and in-hospital death rates related to the most frequent IFIs registered in the national hospital discharge database during 2001-2010. The identified 35,876 IFI cases included candidemia (43.4%), Pneumocystis jirovecii pneumonia (26.1%), invasive aspergillosis (IA, 23.9%), cryptococcosis (5.2%), and mucormycosis (1.5%). The overall incidence was 5.9/100,000 cases/year and the mortality rate was 27.6%; both increased over the period (+1.5%, +2.9%/year, respectively). Incidences substantially increased for candidemia, IA, and mucormycosis. Pneumocystis jirovecii pneumonia incidence decreased among AIDS patients (-14.3%/year) but increased in non-HIV-infected patients (+13.3%/year). Candidemia and IA incidence was increased among patients with hematologic malignancies (>+4%/year) and those with chronic renal failure (>+10%/year). In-hospital deaths substantially increased in some groups, e.g., in those with hematologic malignancies. IFIs occur among a broad spectrum of non-HIV-infected patients and should be a major public health priority.
Keywords: Invasive mycosis; Pneumocystis jirovecii; aspergillosis; candidemia; cryptococcosis; mucormycosis.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
